Downloaded 857 times




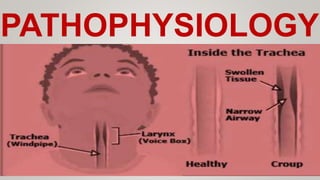








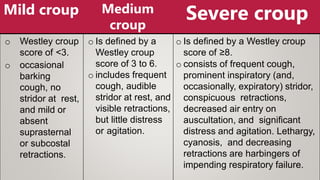












Croup is a respiratory illness that mainly affects young children, characterized by a barking cough and stridor. It is usually caused by viruses like parainfluenza or RSV infecting the larynx and trachea, causing inflammation and swelling that narrows the airway. Symptoms range from mild cough to severe distress. Treatment involves corticosteroids, nebulized epinephrine, humidified air, and hospitalization for children with progressive symptoms or respiratory distress. Croup has an excellent prognosis with near complete recovery in most cases.

















































































