This document discusses the initial management of urethral injuries. It describes the anatomy of the male and female urethra and types of urethral injuries. For anterior urethral injuries, the classic triad of symptoms is outlined and initial investigations and management with suprapubic cystostomy or immediate repair are summarized. Posterior urethral injuries are often associated with pelvic fractures and initial management focuses on hemodynamic stability and associated injuries before addressing the urethra. The document recommends suprapubic cystostomy with possible delayed endoscopic realignment as the standard approach.


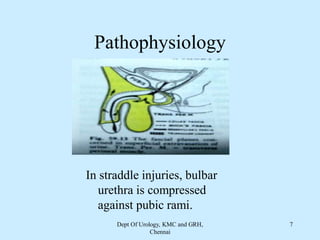







![MANAGEMENT
• SPC alone-
96% develops urethral stricture, which require posterior urethroplasty.
• SPC + Initial Primary Re-alignment
Heals without stricture
Heals with mild stricture [Dilatation + O.I.U]
Eases Subsequent urethroplasty.
• SPC followed by delayed or secondary repair after 3 – 6 months.
Dept Of Urology, KMC and GRH,
Chennai
25](https://image.slidesharecdn.com/gu-trauma-urethra-initialmanagement-210605035139/85/Gu-trauma-urethra-initial-management-25-320.jpg)


























![Benign Prostatic Hyperplasia BPH [Dr. Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/bphedmond-140716213908-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
































































