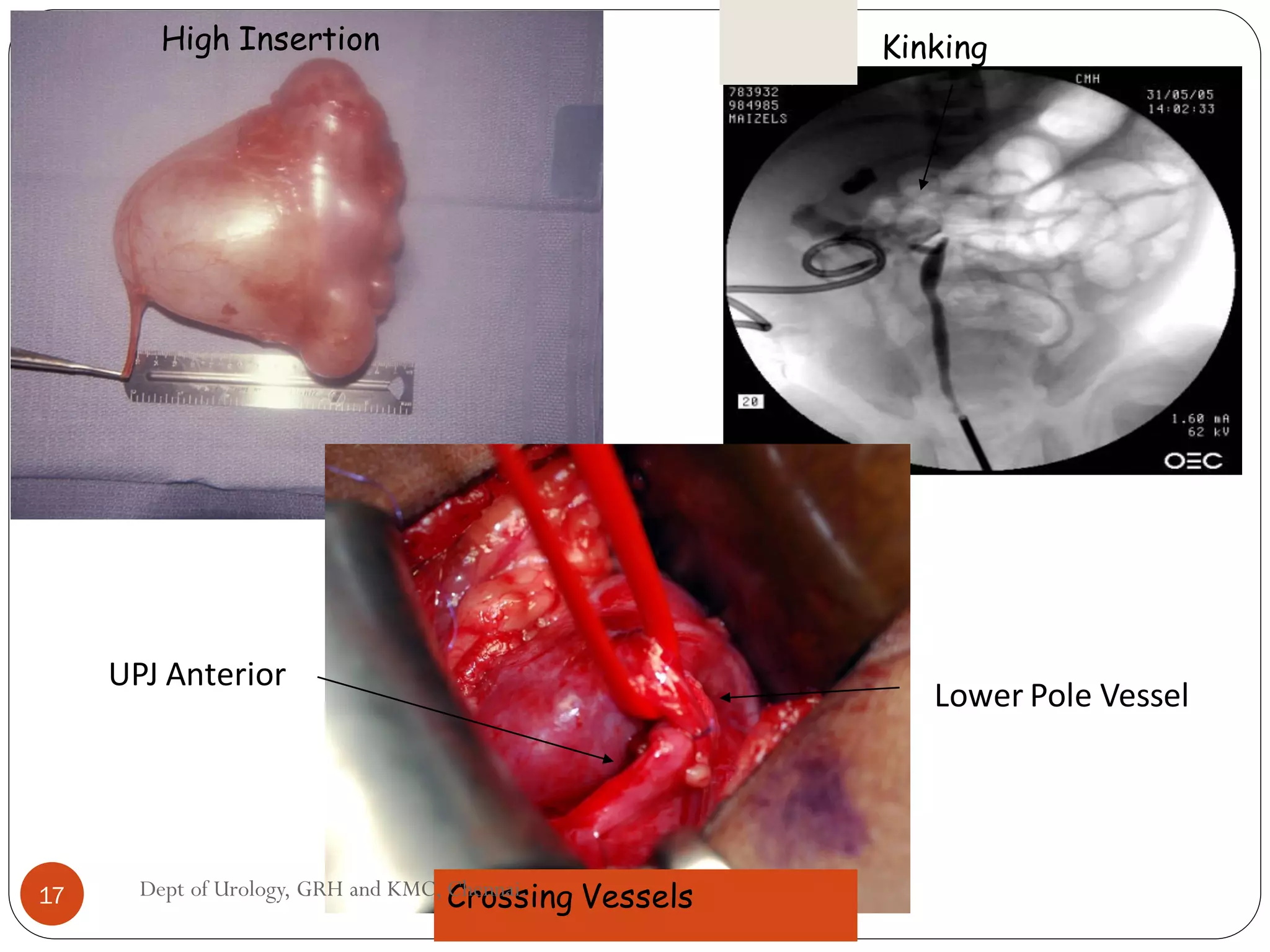
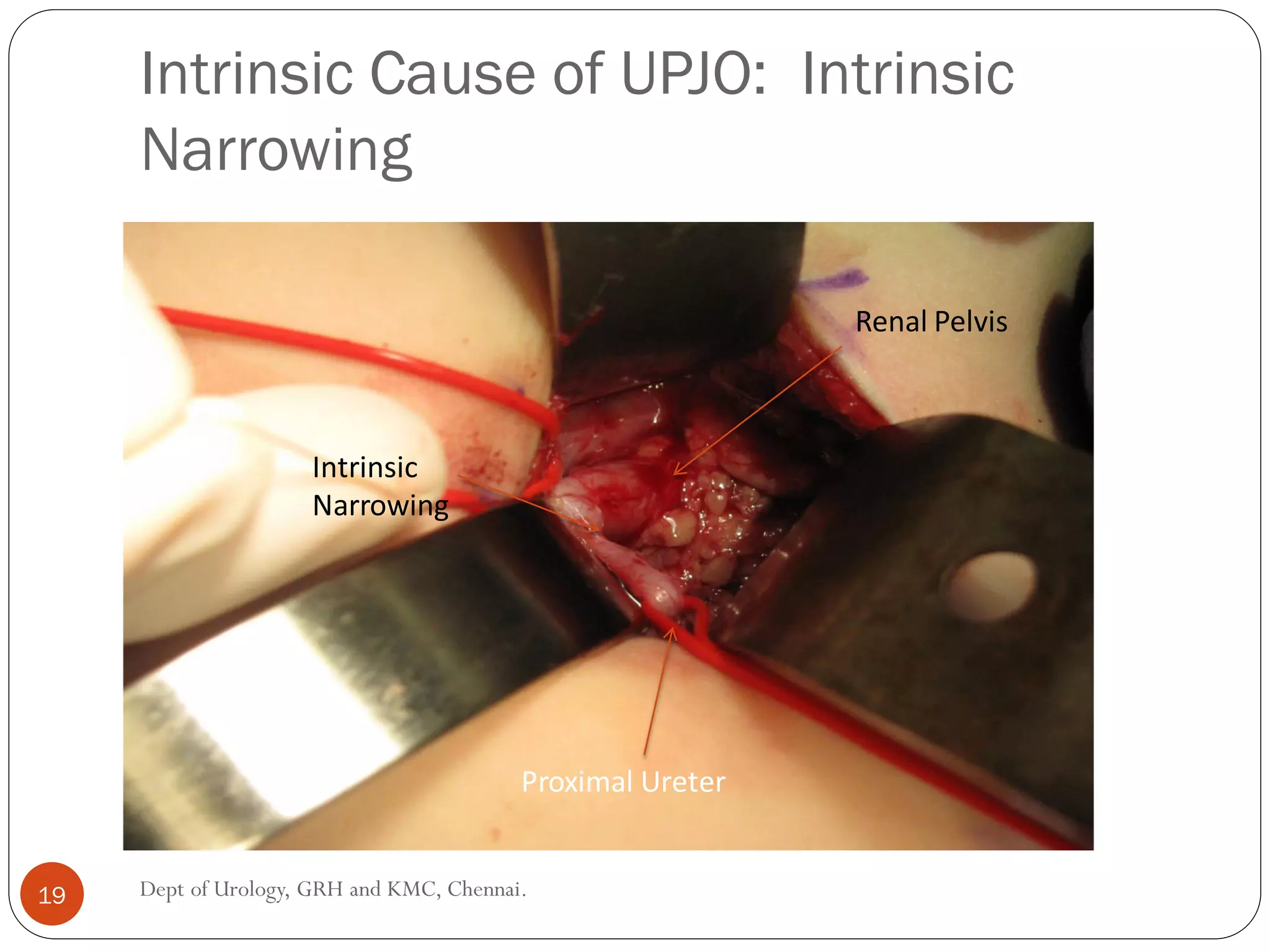
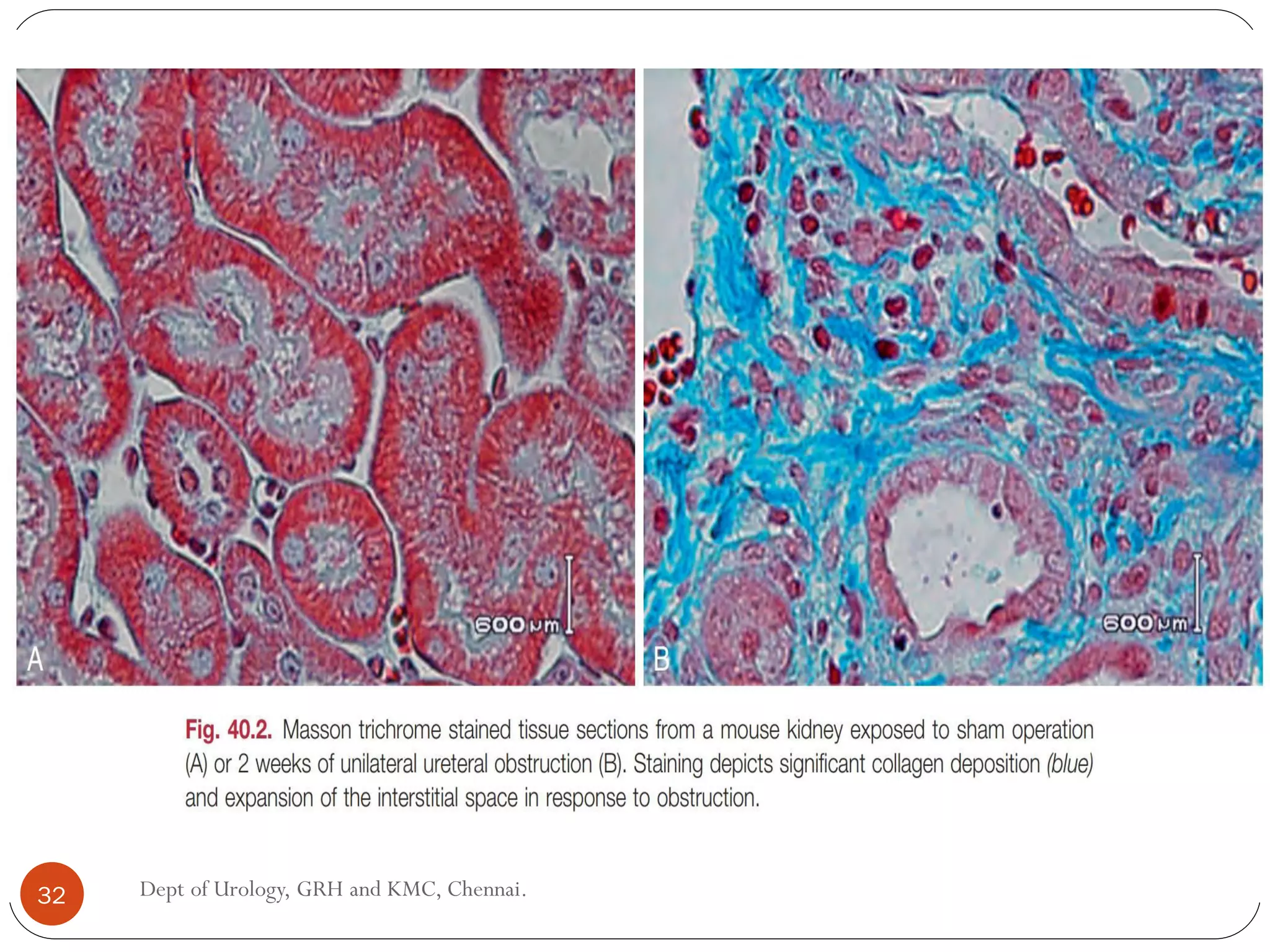
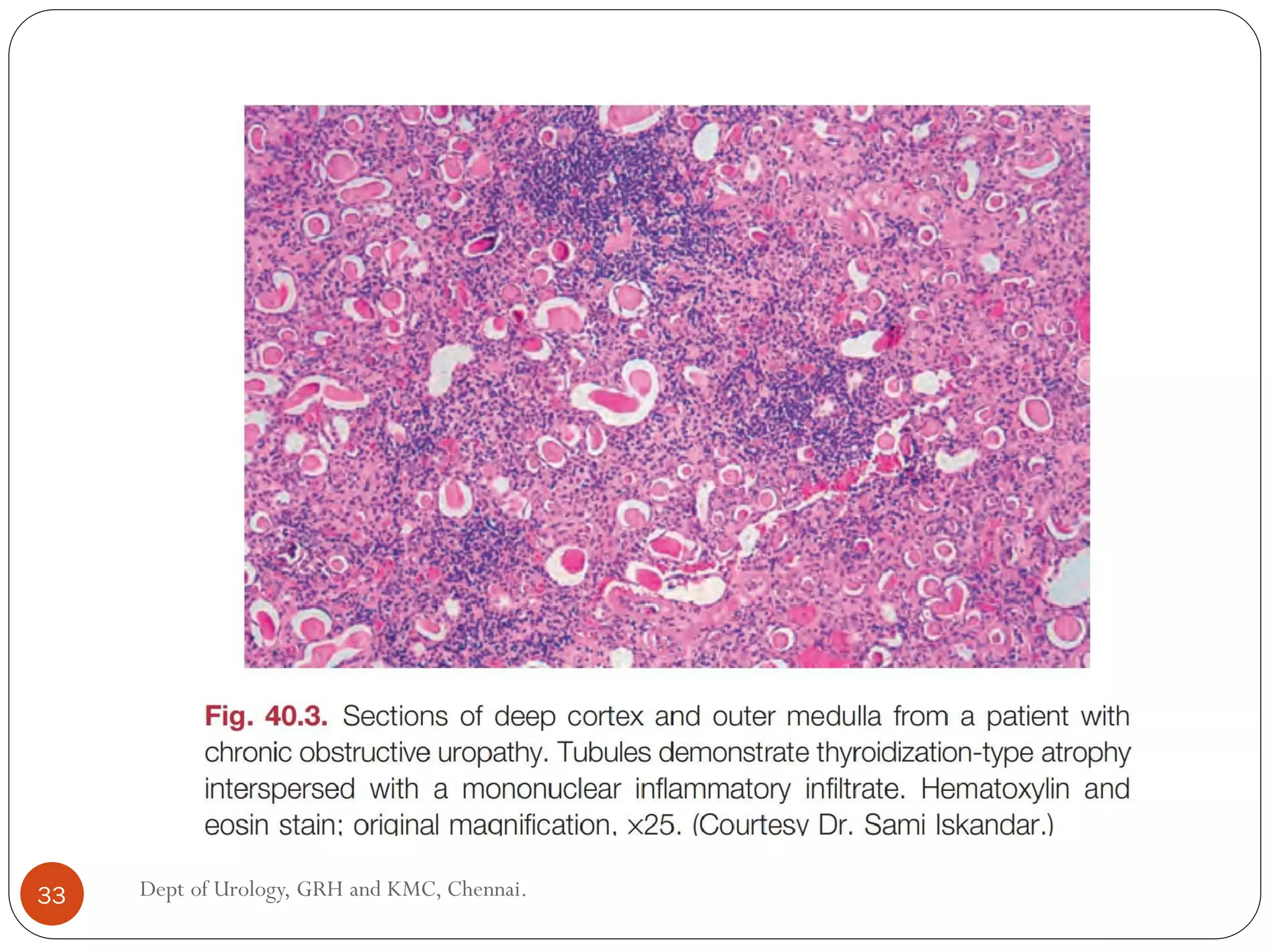
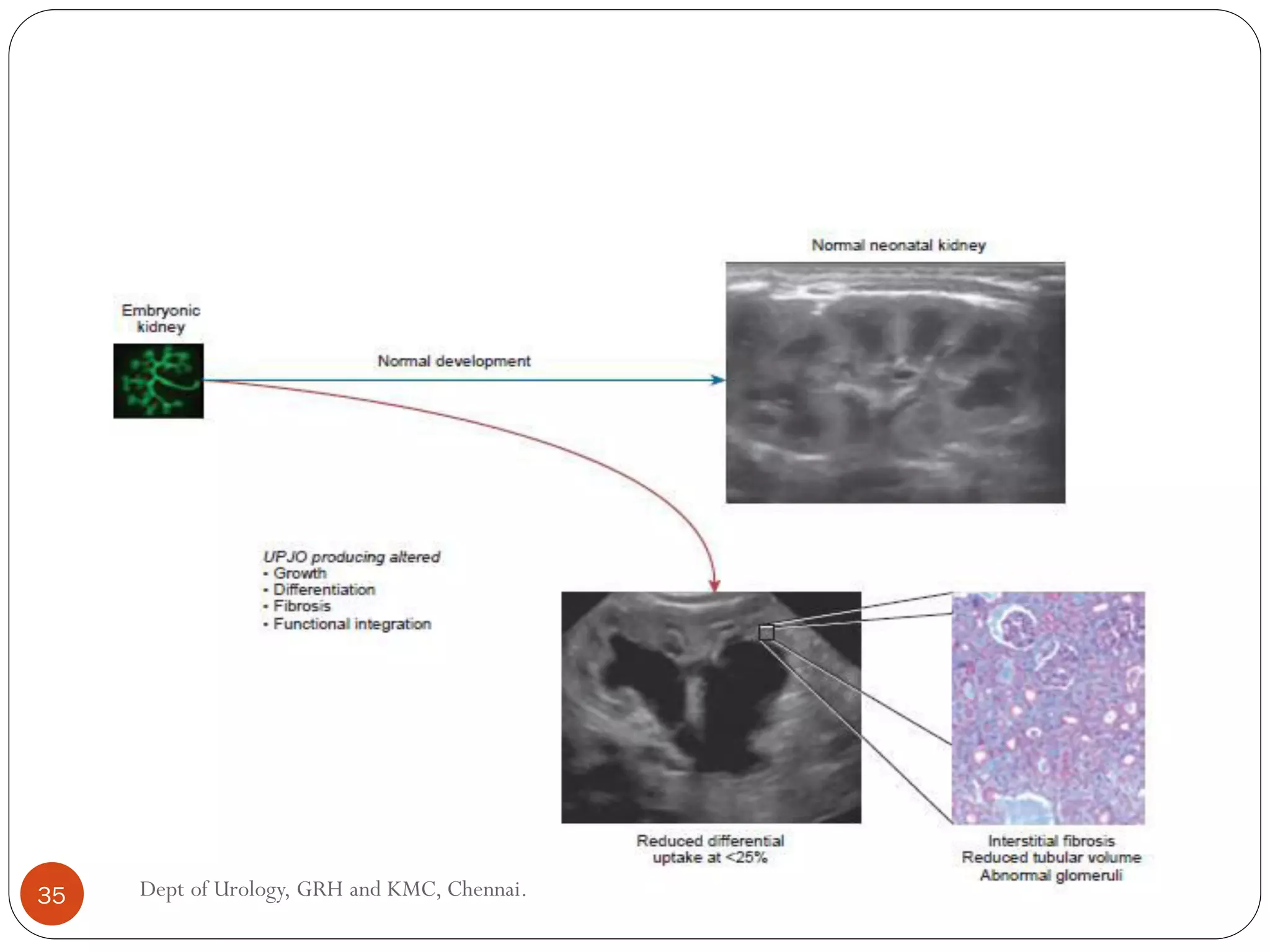
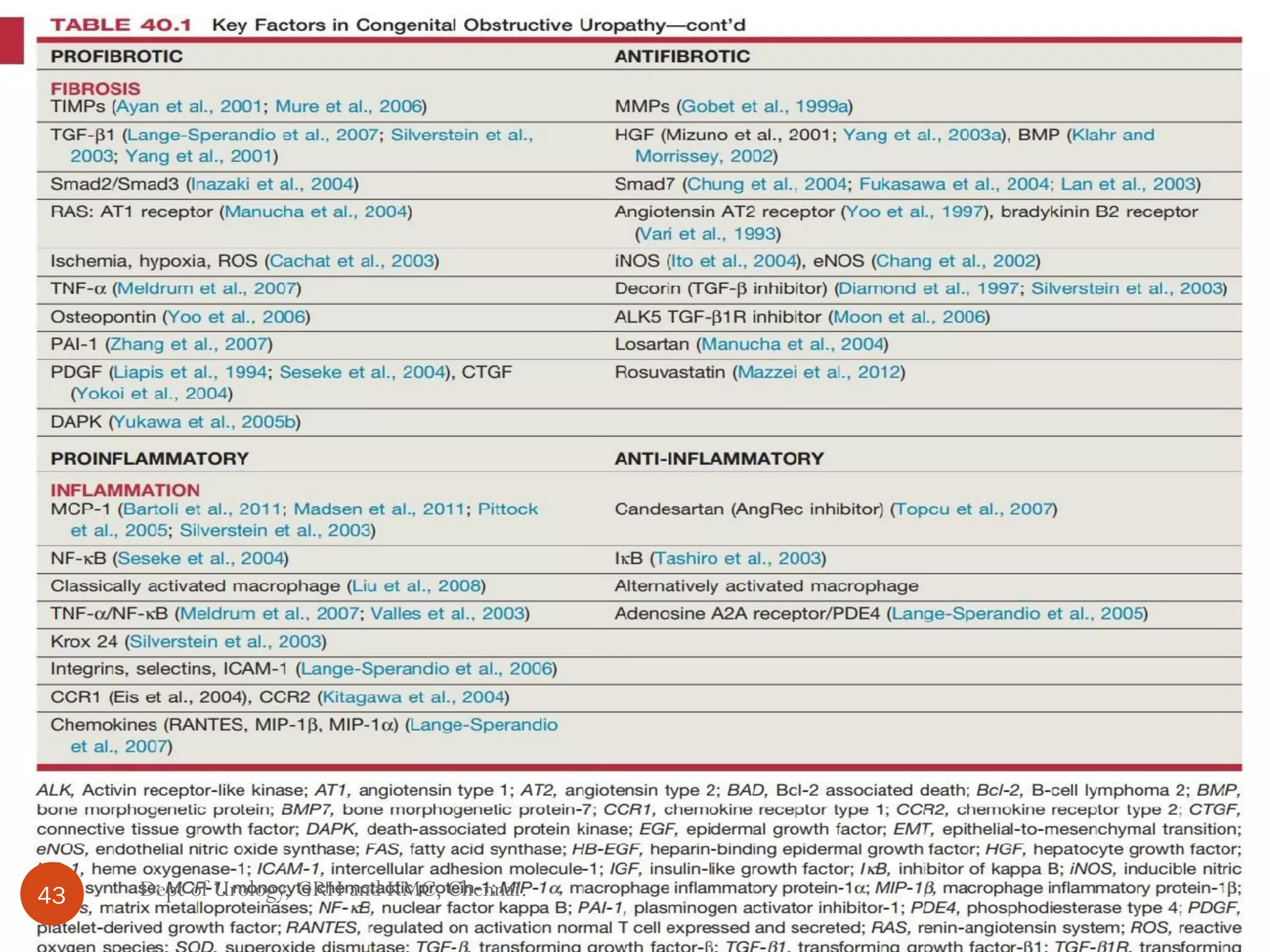
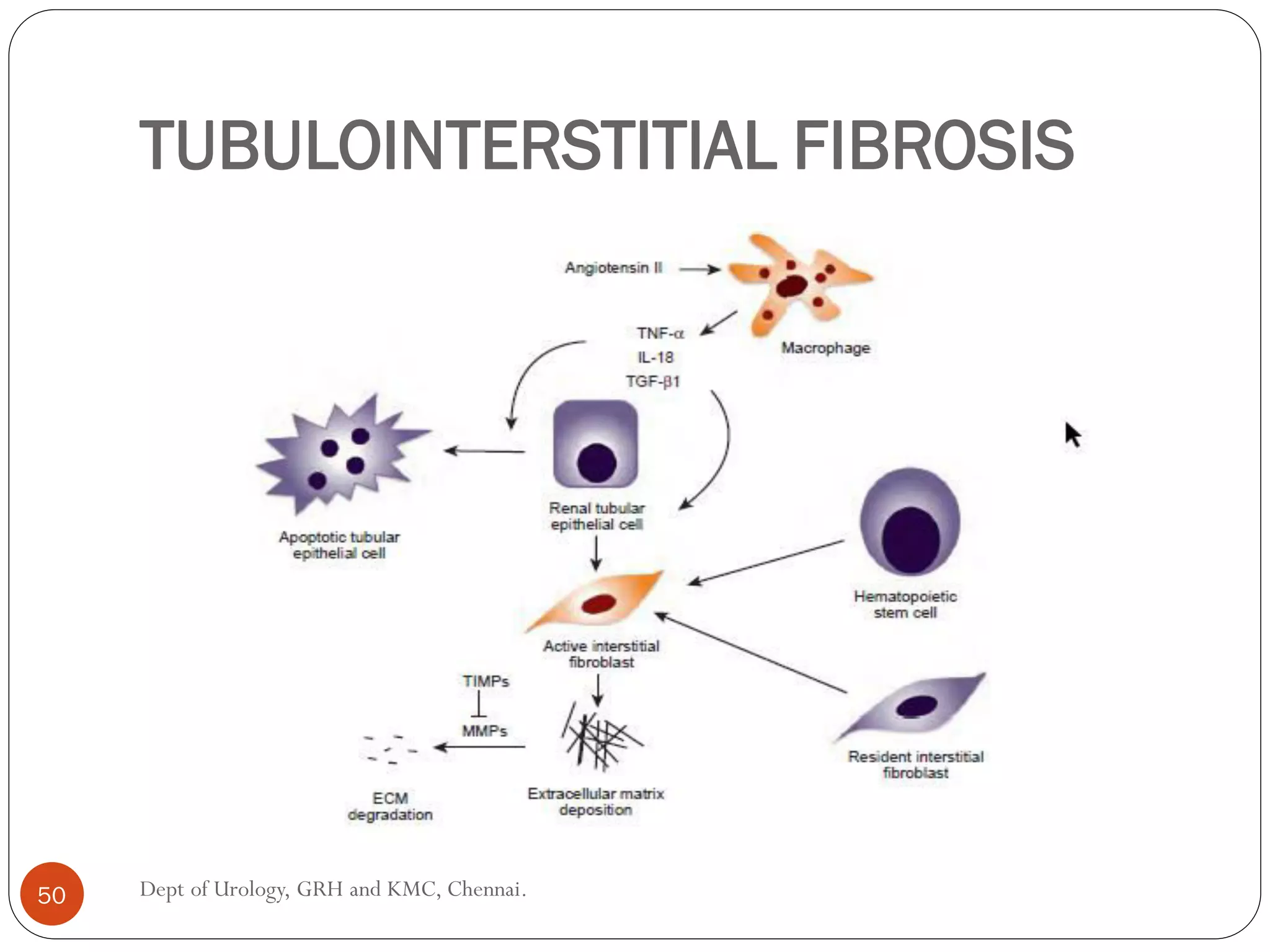
This document discusses congenital pelvi-ureteric junction obstruction (PUJO). It covers the etiology, pathogenesis, pathological changes, and clinical presentation of PUJO. The main causes of PUJO are believed to be intrinsic abnormalities at the pelvi-ureteric junction that cause an aperistaltic segment and prevent normal urine flow. This can result from developmental arrest or incomplete recanalization. PUJO can also be caused by external compression from aberrant vessels. Longstanding obstruction leads to hydronephrosis, tubular dilation, interstitial fibrosis and loss of renal function over time. Clinically, PUJO usually presents with hydronephrosis in infants and children.




































































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)

















