Downloaded 152 times

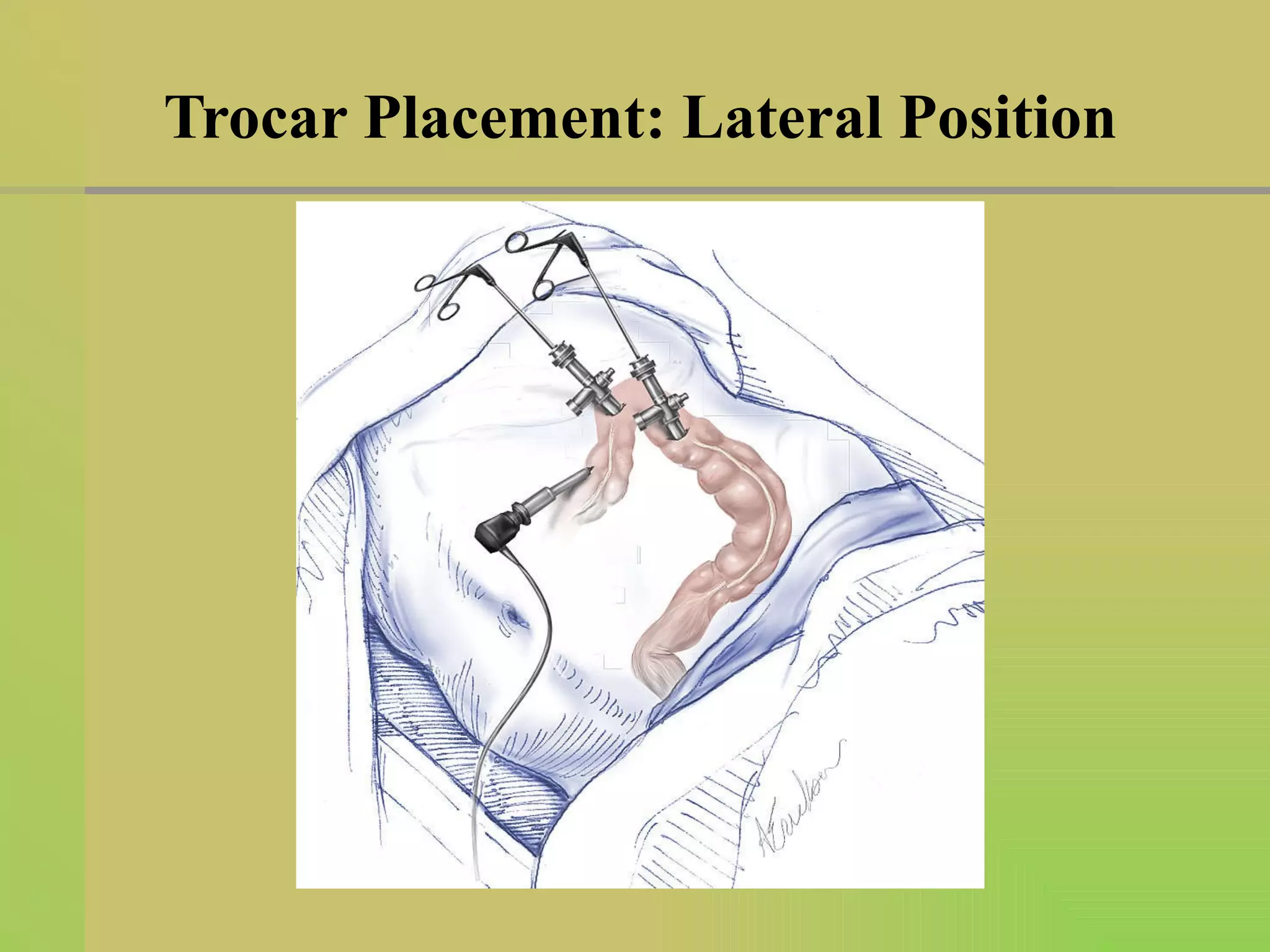
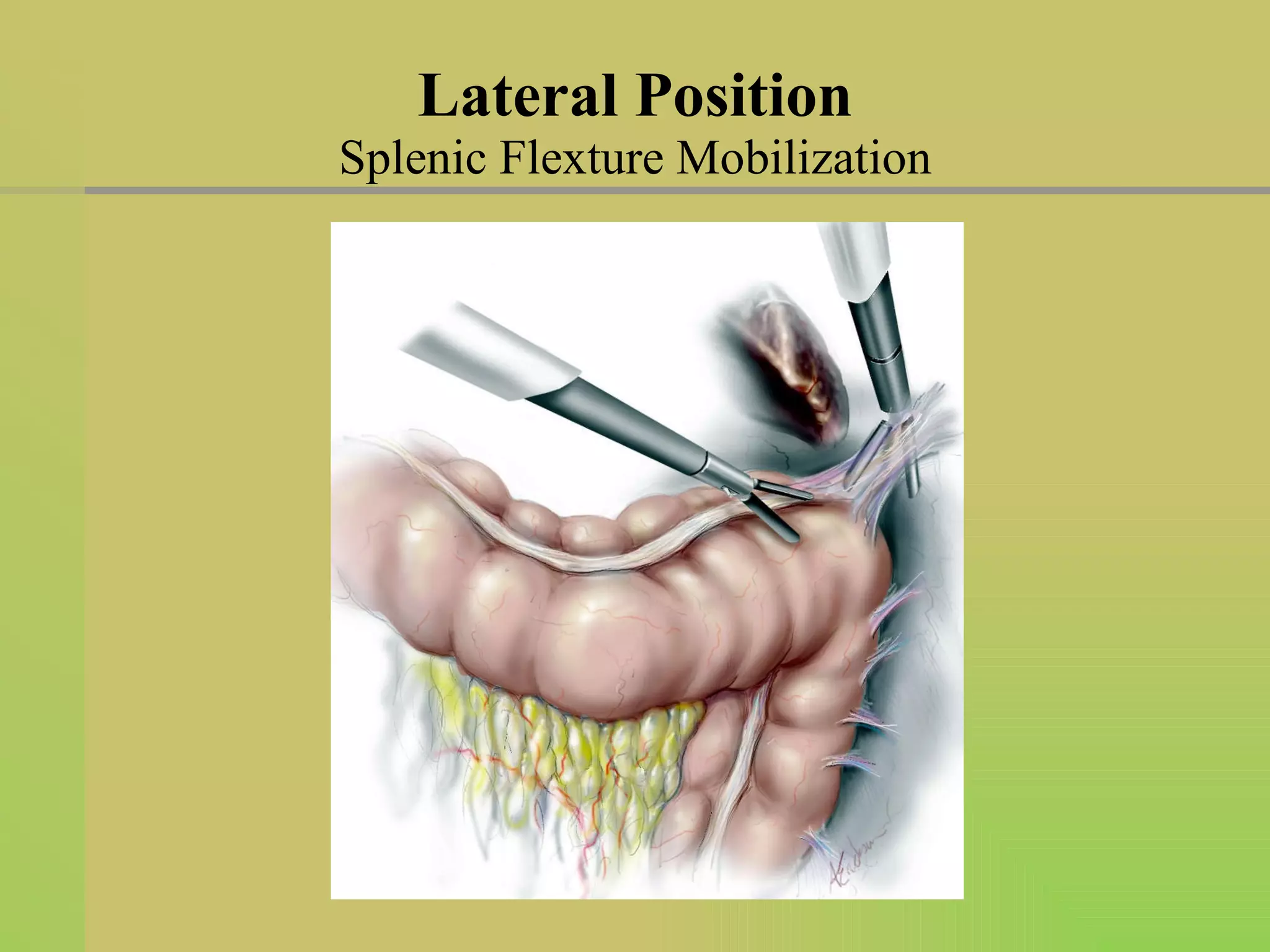
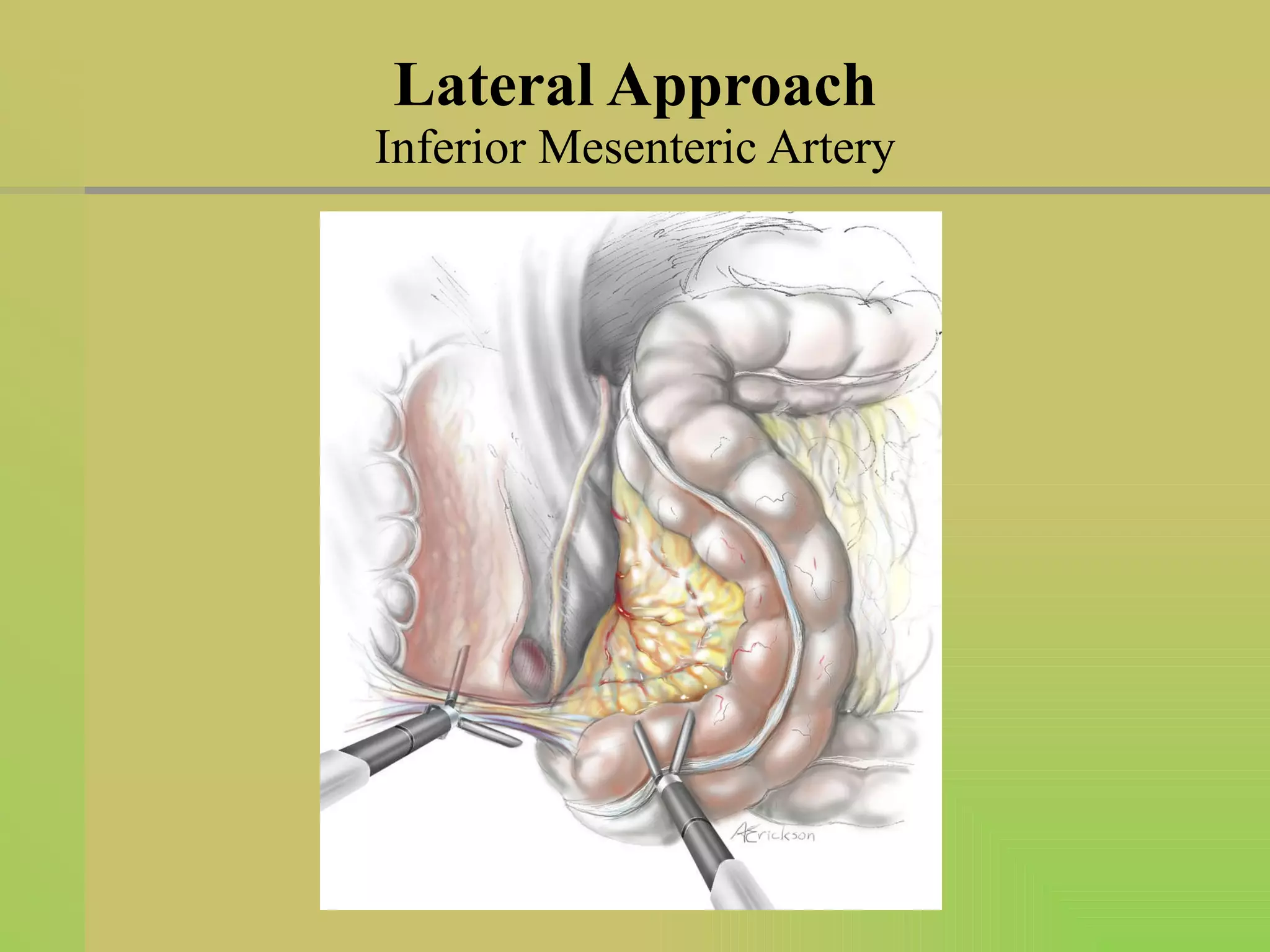
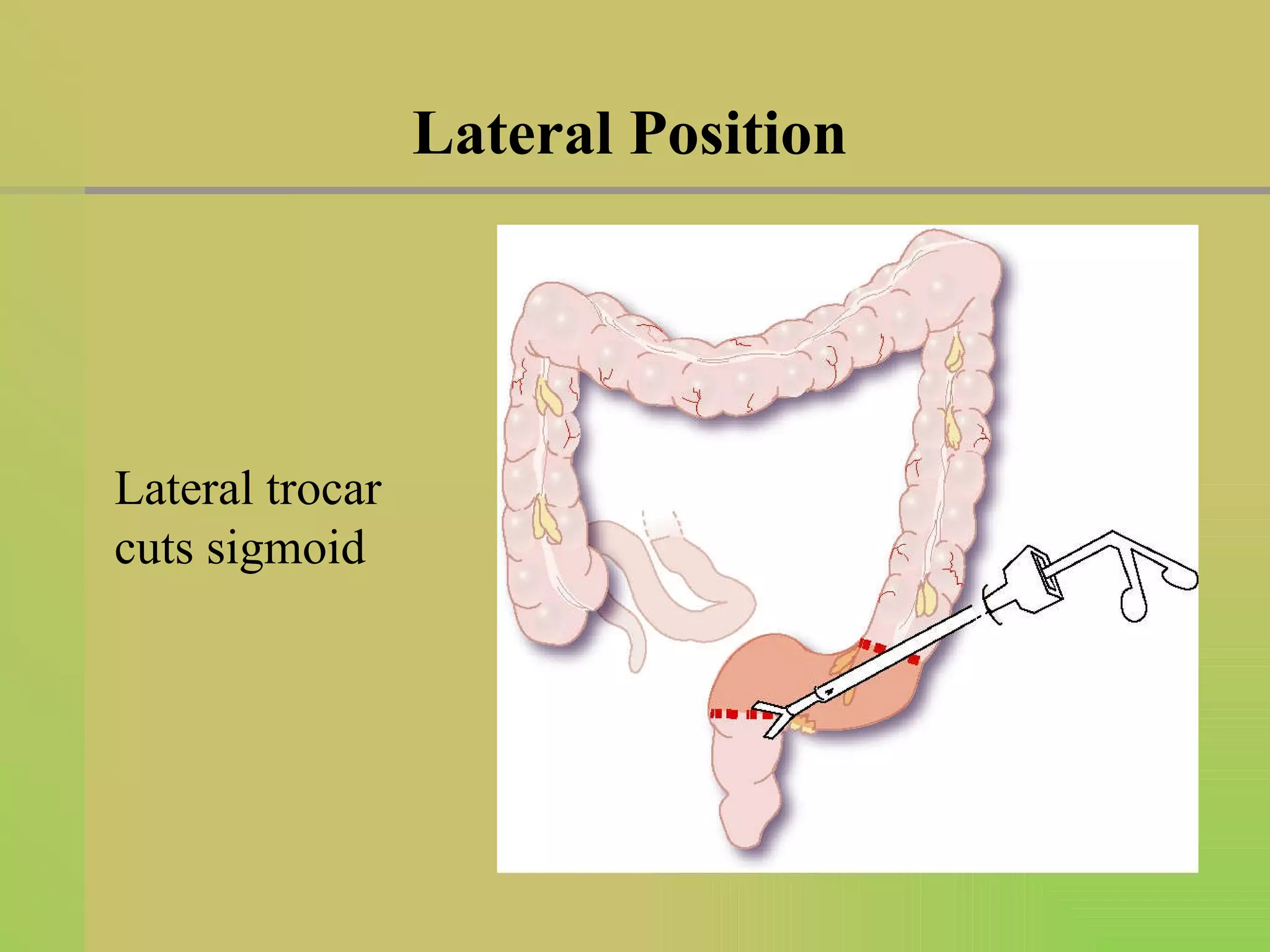
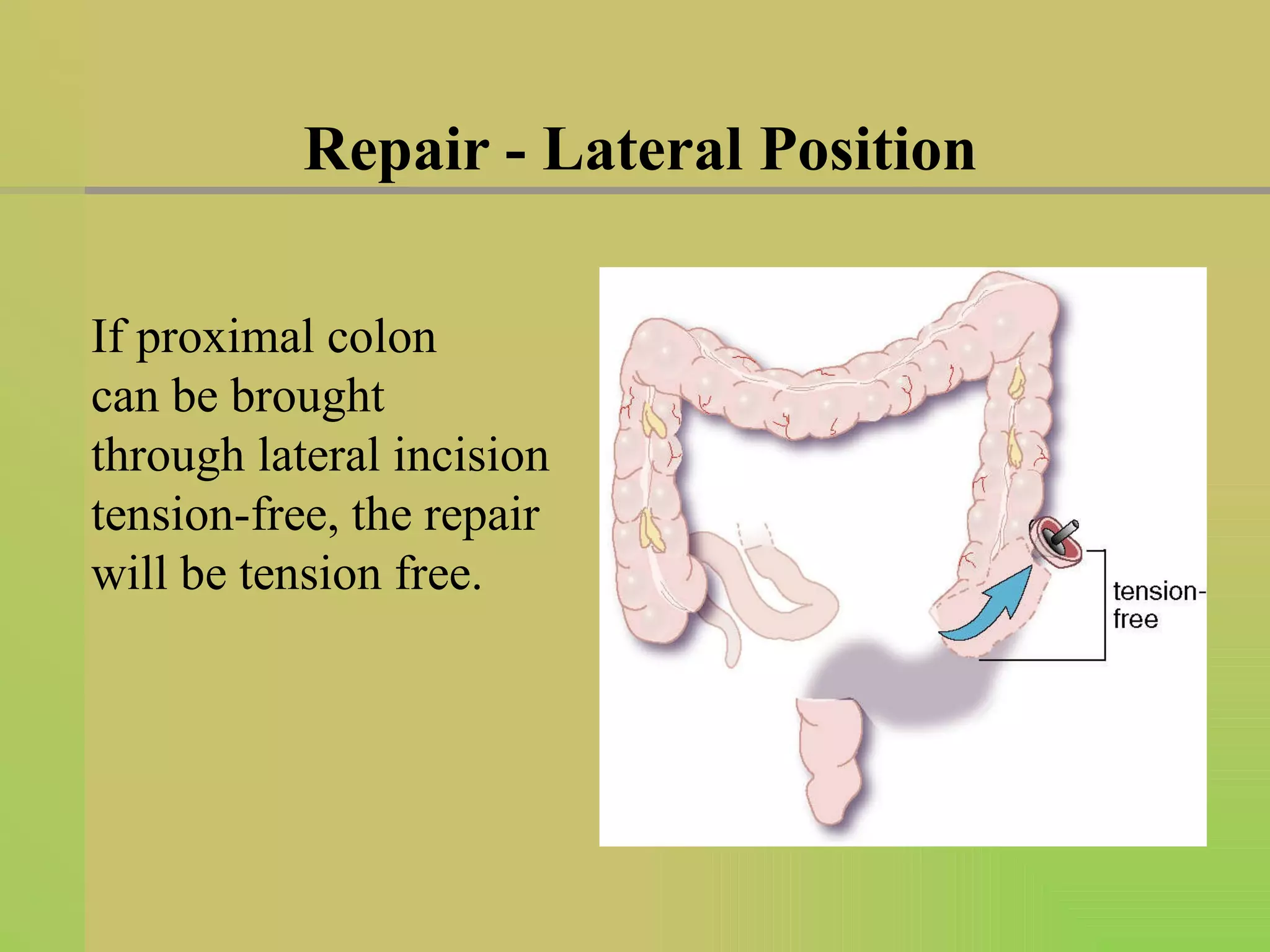
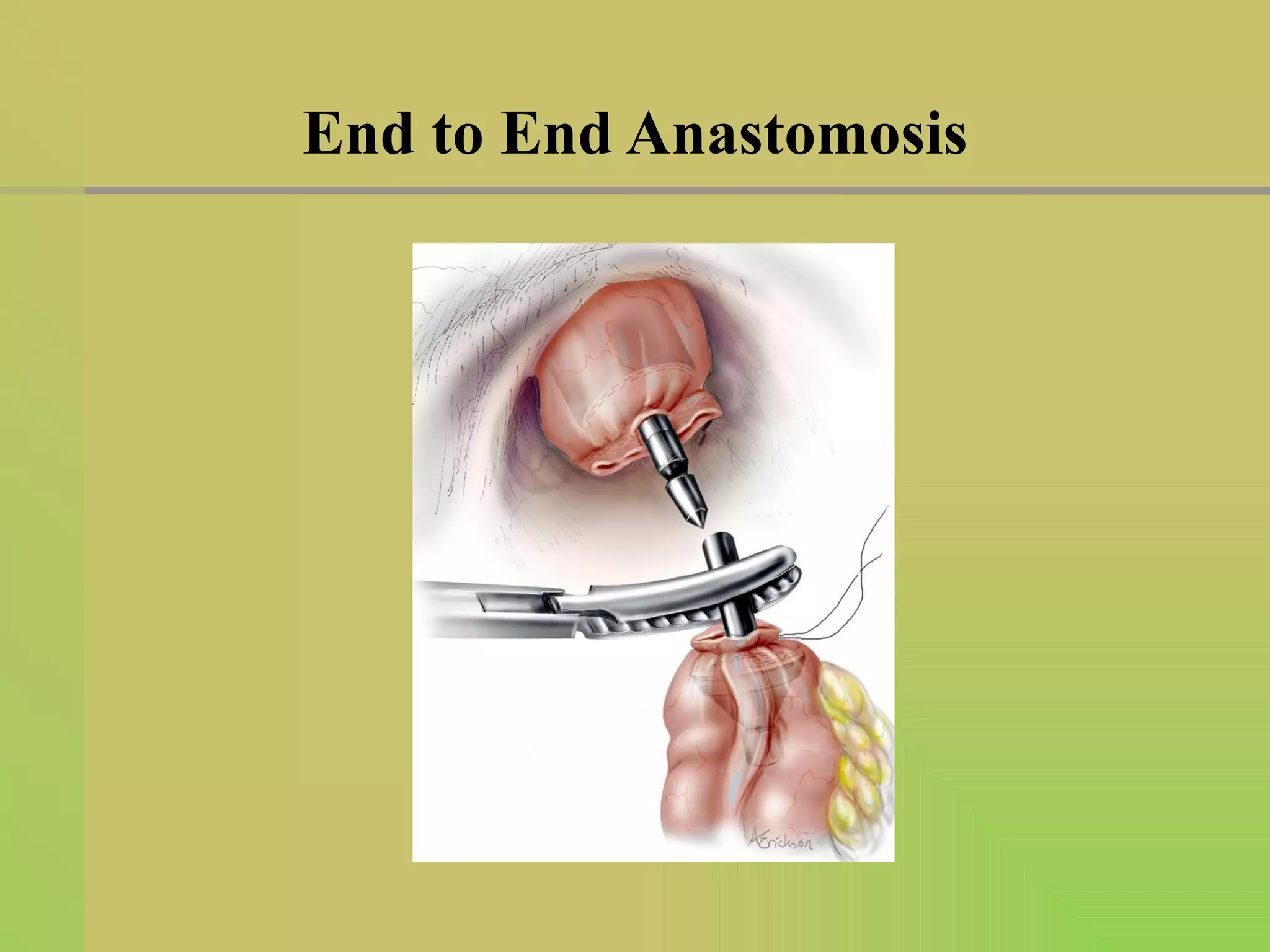

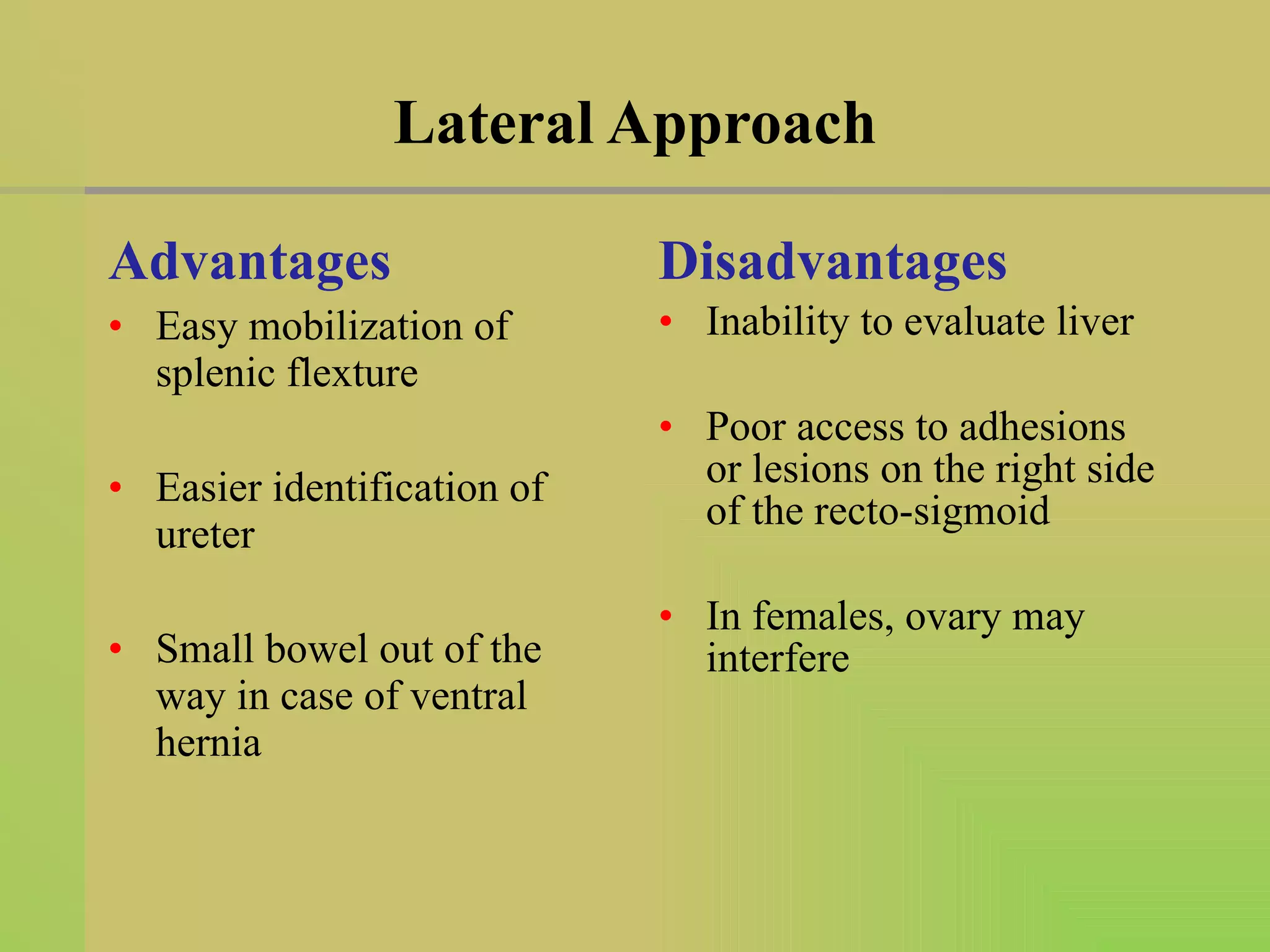
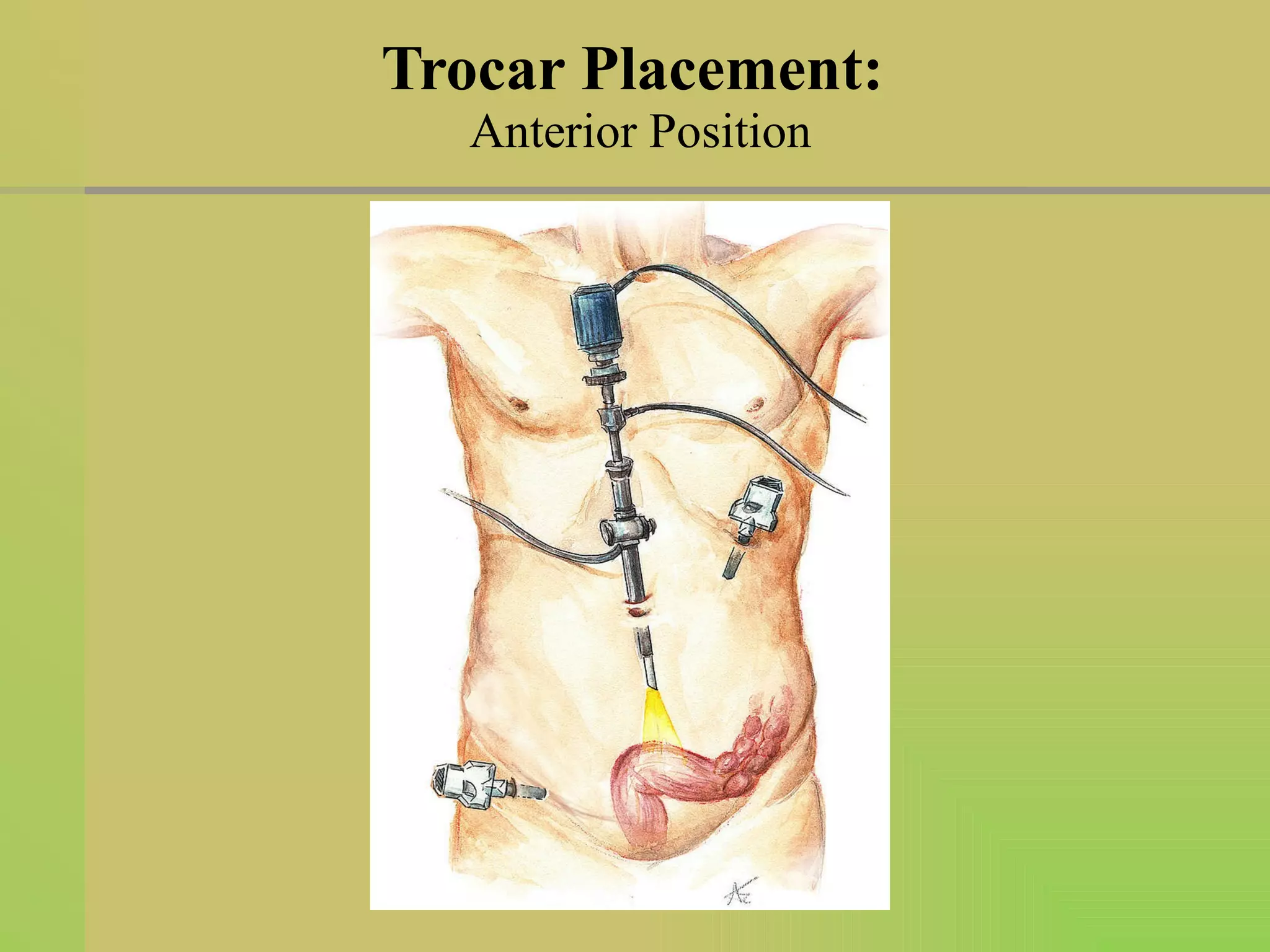
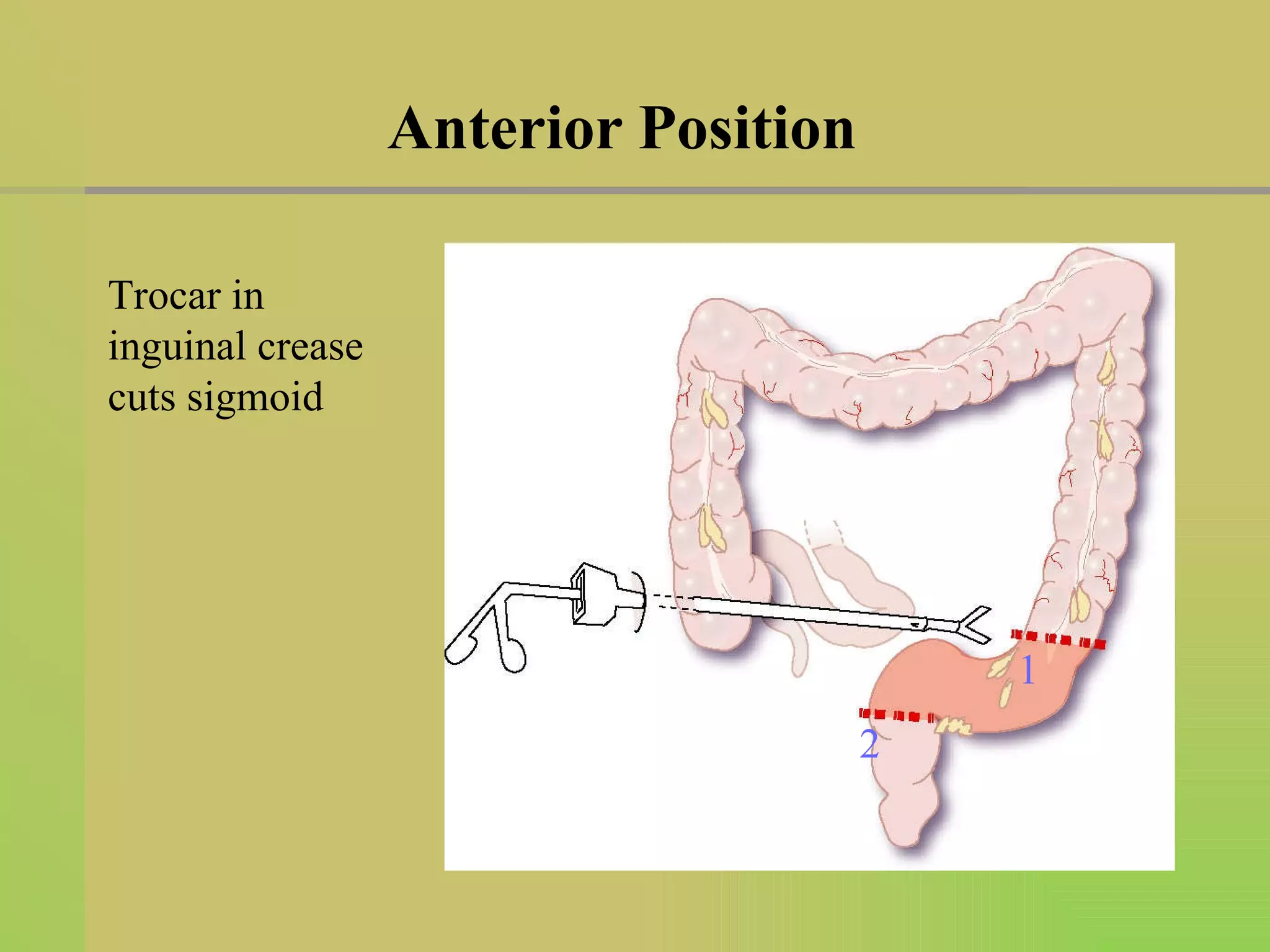
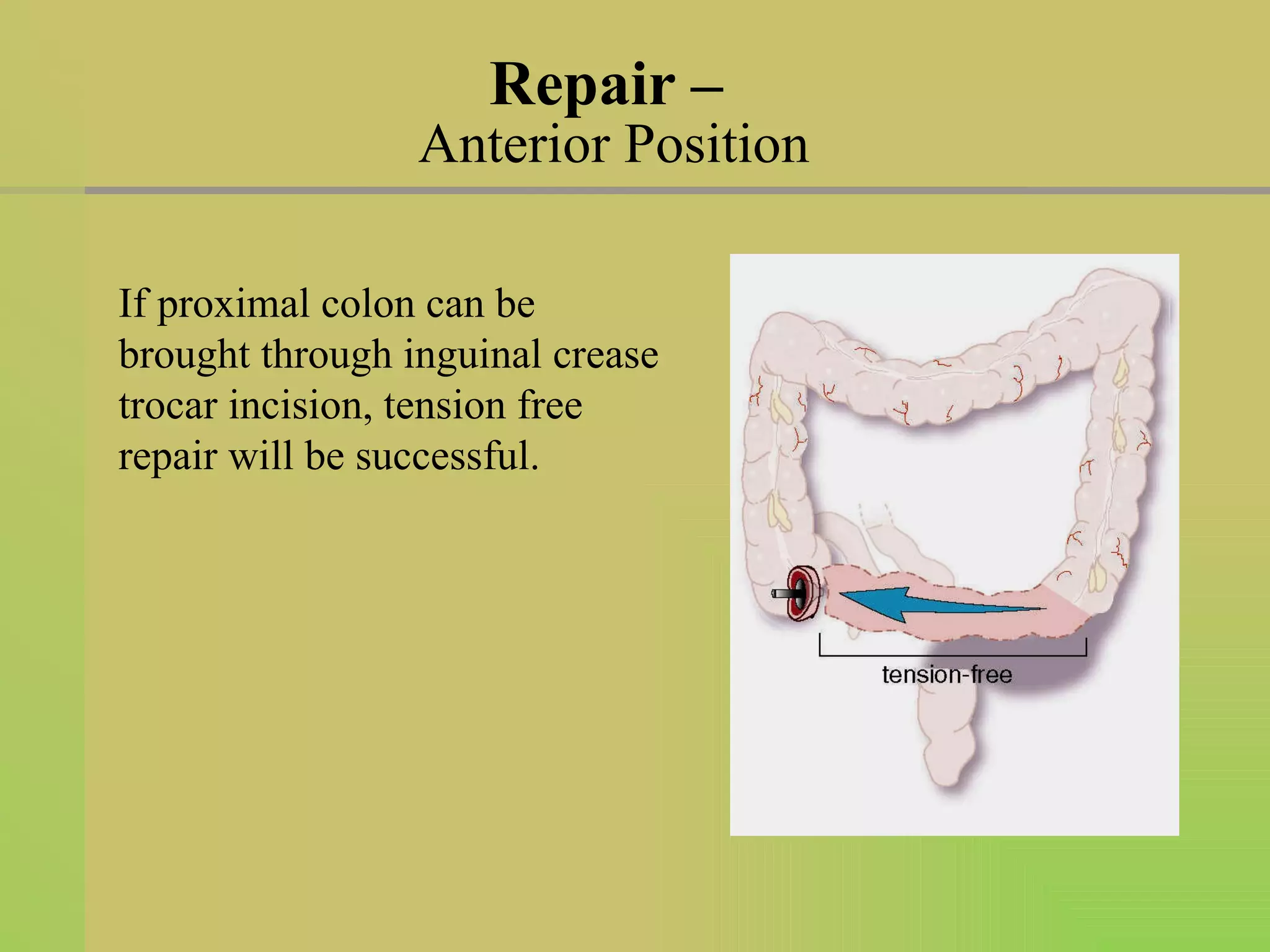

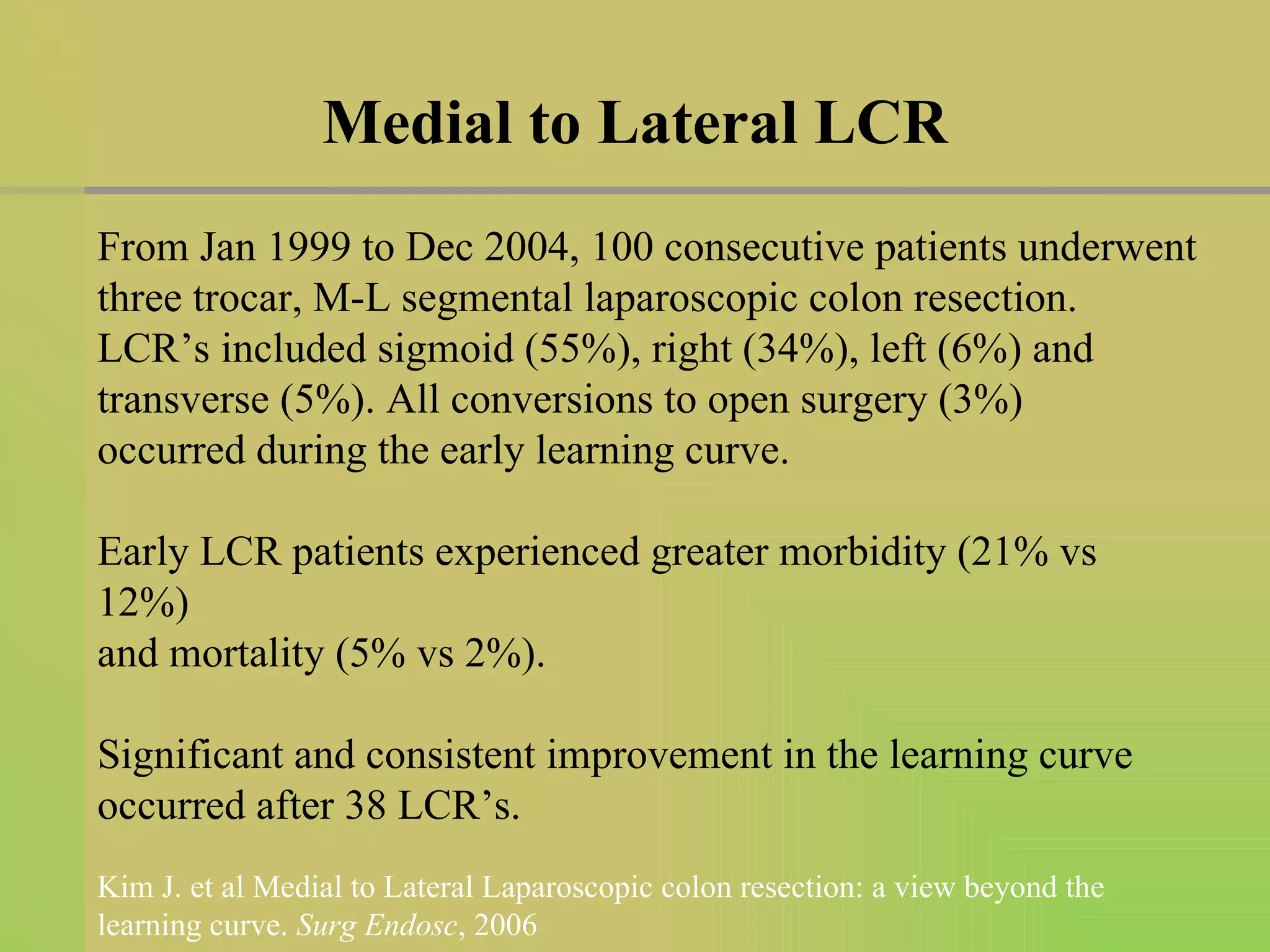
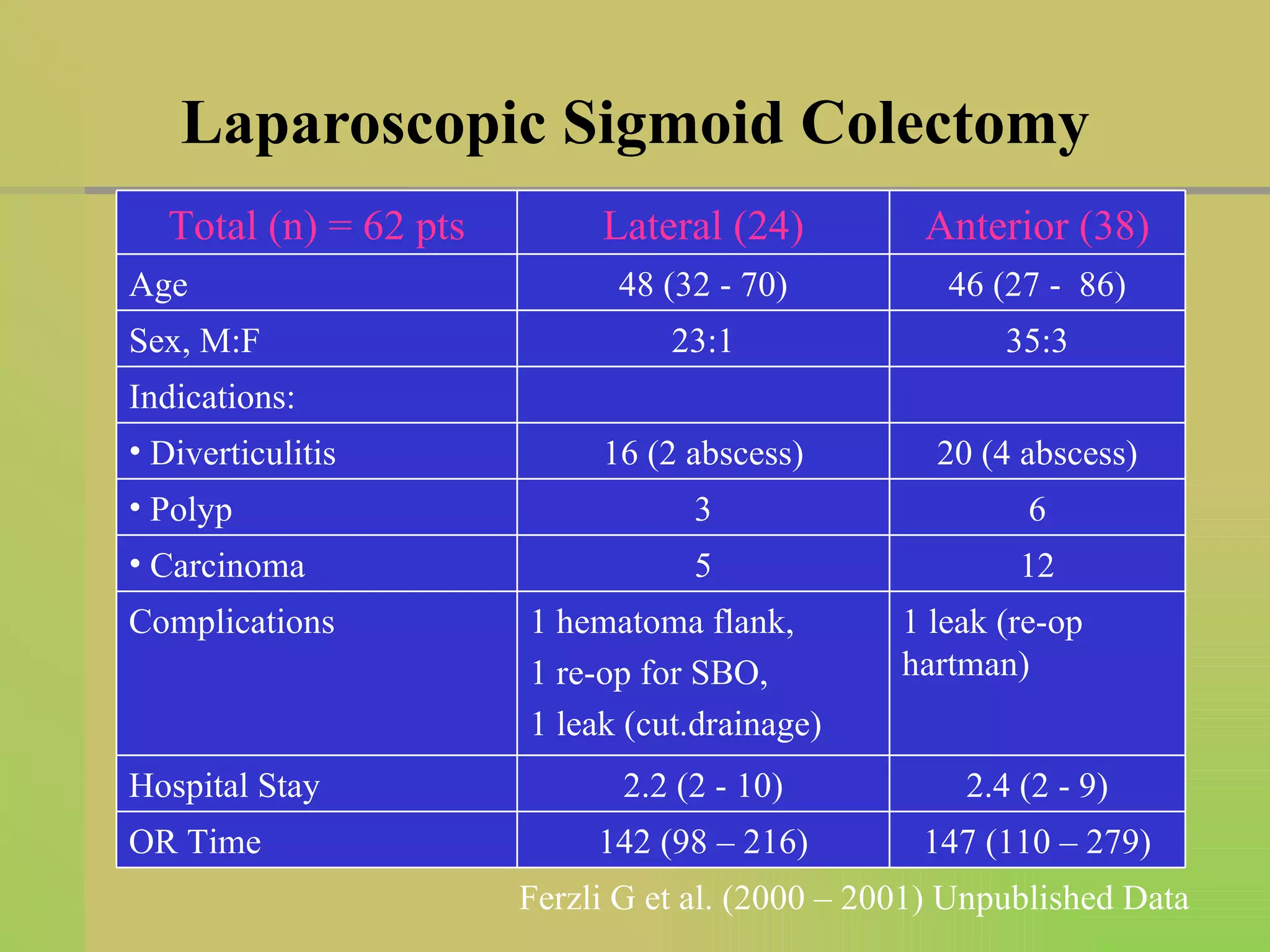
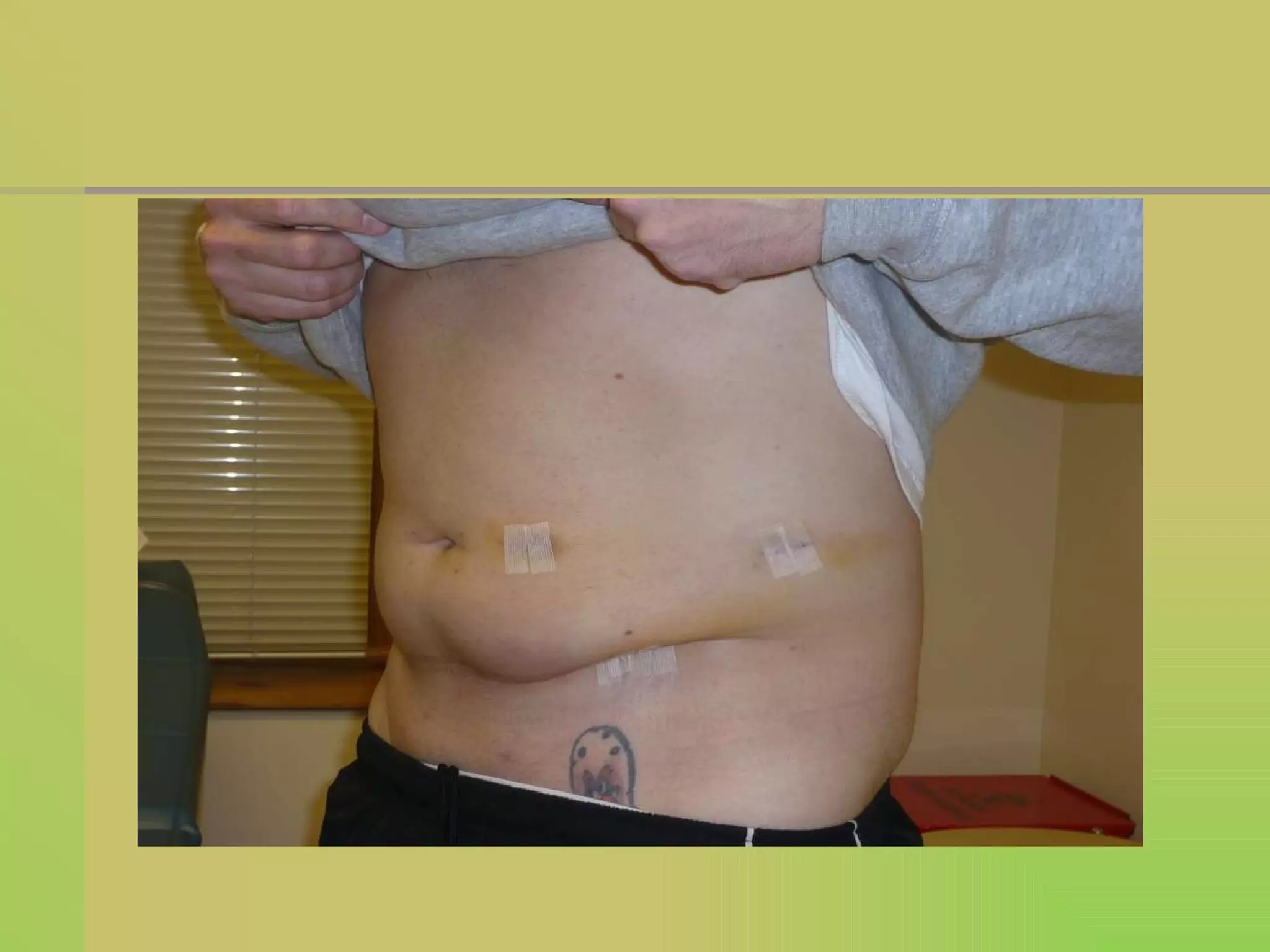


The document discusses different approaches for performing a laparoscopic sigmoid colon resection surgery. It describes the lateral and anterior patient positioning approaches. For the lateral approach, the patient is positioned on their right side and trocars are placed in a triangular configuration. This approach allows for easy mobilization of the splenic flexure but has disadvantages like poor access to the right side of the rectosigmoid area. The anterior approach involves positioning the patient supine and placing trocars in a semicircular configuration above the sigmoid colon. Both approaches aim to bring the proximal colon through the incision sites to allow for a tension-free anastomosis repair. Data on outcomes from 62 patients undergoing either the lateral or anterior approach are also presented.























































































