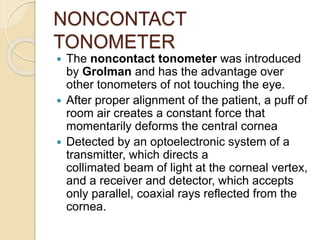
Tonometry is used to measure intraocular pressure. There are two main types - indentation and applanation tonometers. The Schiotz indentation tonometer, introduced in 1905, made tonometry a routine clinical test. It measures indentation of the eye to determine pressure. Applanation tonometers flatten a portion of the cornea and relate this to intraocular pressure. The Maklakoff applanation tonometer from 1885 was an early prototype. The Goldmann applanation tonometer, introduced in 1954, is now the gold standard and measures the force needed to flatten a standard corneal area. Recent advances include non-contact tonometry using air puffs and improved accuracy and portability of applanation devices.