Digital Tonometry
Method ofestimating the Intraocular pressure by gently pressing the index finger
against the globe
Method
- Ask the patient to look down
- Place the tip of index finger on closed eyelids above superior tarsal plate
- Press the globe (indent) with the each finger one by one and feel the
compliance with the other finger, one by one.
5.
Interpretation
● Normal -indents easily, firm to touch
● High IOP - Stony Hard
● Low IOP- Soft
ALWAYS COMPARE BOTH EYES
Practical Tip for Residents
- Do the digital tonometry & compare it with NCT/AT
6.
Advantage
Quick, No costinvolved
Easy
- Practical Use: To assess IOP in OPD where tonometers are not available
- Post operative patients where you would avoid touching the cornea
- Post PK & Corneal Ulcer patients
Disadvantage
- Subjective
- Inaccurate
- Unreliable
7.
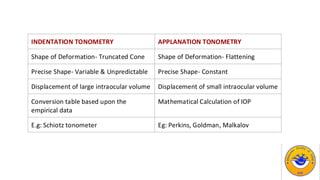
INDENTATION TONOMETRY APPLANATIONTONOMETRY
Shape of Deformation- Truncated Cone Shape of Deformation- Flattening
Precise Shape- Variable & Unpredictable Precise Shape- Constant
Displacement of large intraocular volume Displacement of small intraocular volume
Conversion table based upon the
empirical data
Mathematical Calculation of IOP
E.g: Schiotz tonometer Eg: Perkins, Goldman, Malkalov
8.
Goldmann Applanation Tonometry
Imbert– Fick’s Law*
External Force against a sphere equals the pressure in the
sphere multiplied by the area flattened by external
force
W = P X A
9.
Goldmann Applanation Tonometry
ApplanatingSurface should be
● Dry
● Perfectly Flexible
● Infinitely thin
But Cornea is not a perfect surface, So
We modify the formula as
W = P X A
to
W + S = P X A + B
S = surface tension due to moisture (Force of capillary attraction between the tear film & the cornea)
B = force to bend the cornea due to lack of flexibility/ Corneal rigidity
10.
The internal areais achieved when external applanating diameter is 3.06mm.
● Very minimal amount of displacement is there
● Tip exerts minimal Pressure
● Ocular rigidity doesnot affect much
ADVANTAGES OF THE FORMULA
11.
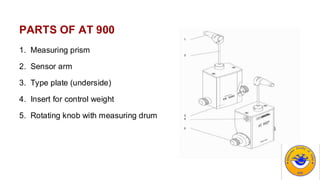
PARTS OF AT900
1. Measuring prism
2. Sensor arm
3. Type plate (underside)
4. Insert for control weight
5. Rotating knob with measuring drum
12.
PROCEDURE
• Press headfirmly against chin against forehead rest & look straight.
• Breathe normally, do not hold your breath or any valsalva procedure & blink prior to
measurement to moisten cornea.
• Position patient’s head with forehead rest well above eyebrows, allowing raising of
eyebrows.
•Anesthetic & fluorescein separately are placed in inferior cul-de-sac.
•Blue filter is used with 10 X magnification. Maximum illumination & Maximum beam
height is used
•Tension knob set at approximate IOP that the patient may be having.
13.
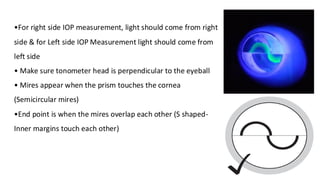
•For right sideIOP measurement, light should come from right
side & for Left side IOP Measurement light should come from
left side
• Make sure tonometer head is perpendicular to the eyeball
• Mires appear when the prism touches the cornea
(Semicircular mires)
•End point is when the mires overlap each other (S shaped-
Inner margins touch each other)
14.
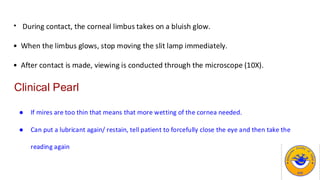
• During contact,the corneal limbus takes on a bluish glow.
• When the limbus glows, stop moving the slit lamp immediately.
• After contact is made, viewing is conducted through the microscope (10X).
Clinical Pearl
● If mires are too thin that means that more wetting of the cornea needed.
● Can put a lubricant again/ restain, tell patient to forcefully close the eye and then take the
reading again
15.
Limitations
Ocular surface related
Cornealthickness deviation from average 520 micron, causes error
● Thicker cornea overestimates IOP
● Thinner cornea underestimates IOP
Scarred corneas - applanating area diameter 3.06 mm is not achieved, giving rise to
errors. Tonopen more reliable.
● ·Dry eyes , causes under staining , narrower meniscus
16.
Technique related
● Fluoresceinamount inappropriate - overstaining leads to wider meniscus with IOP
overestimation & vice versa
● Prolonged contact - causes corneal injury (toe print) & decreases IOP over period of
minutes (pseudo-facility)
● Elevating eyes more than 15° above horizontal meridian causes overestimation
● Widening lid fissure excessively, lid squeezing, breath holding or constrictive neck
clothing like tie can cause overestimation of IOP
17.
Disinfection
● Wiping with70% isopropyl alcohol swabs
● Putting it in 3% diluted sodium hypochlorite or 3 % H2O2 for 5-15 min followed by
rinsing with normal saline, residual disinfectant causes corneal abrasion in patients
eye
18.
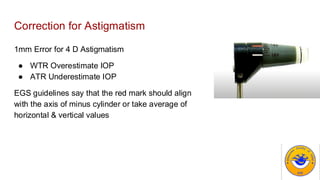
Correction for Astigmatism
1mmError for 4 D Astigmatism
● WTR Overestimate IOP
● ATR Underestimate IOP
EGS guidelines say that the red mark should align
with the axis of minus cylinder or take average of
horizontal & vertical values
19.
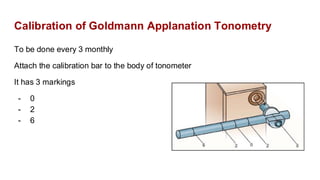
Calibration of GoldmannApplanation Tonometry
To be done every 3 monthly
Attach the calibration bar to the body of tonometer
It has 3 markings
- 0
- 2
- 6
20.
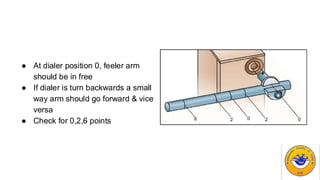
● At dialerposition 0, feeler arm
should be in free
● If dialer is turn backwards a small
way arm should go forward & vice
versa
● Check for 0,2,6 points
21.
Perkins tonometer
- Usessame GAT
- Light source is powered by battery & Can
be used in both horizontal & vertical
positions
- Portable
- Especially useful for EUA & Infants and
patients who could not sit at slit lamp
22.
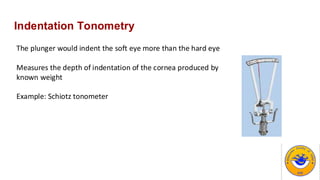
Indentation Tonometry
The plungerwould indent the soft eye more than the hard eye
Measures the depth of indentation of the cornea produced by
known weight
Example: Schiotz tonometer
23.
Limitations
- Can injurethe cornea
- Error due to High IOP (Thyroid Ophthalmopathy)
- Source of error: Manufacturing defects like difference in the size, weight & shape
of footplate
- Error due to accommodation (Contraction of ciliary muscle)
- Inc in Aqueous Outflow (Pulling the TM): Decrease in IOP
- Steep & thicker corneas have false high IOP
24.
Falsely high IOPdue to high Ocular
Rigidity
- High Hypermetropia
- Chronic Glaucoma
- Vasoconstrictor therapy
- ARMD
Falsely Low IOP due to low Ocular
Rigidity
- High Myopia
- RD
- Vasodilator therapy
- Miotic therapy
25.
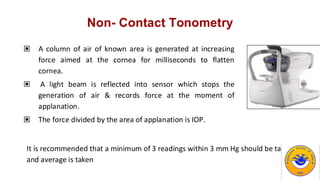
Non- Contact Tonometry
▣A column of air of known area is generated at increasing
force aimed at the cornea for milliseconds to flatten
cornea.
▣ A light beam is reflected into sensor which stops the
generation of air & records force at the moment of
applanation.
▣ The force divided by the area of applanation is IOP.
It is recommended that a minimum of 3 readings within 3 mm Hg should be taken
and average is taken
26.
Disadvantage
- Shields etal showed that poor co-
relation with Goldman’s AT at higher
intraocular pressure.
- Large, not very portable, expensive.
- Inaccurate in eyes whose corneas are
irregular, scarred, edematous, or
astigmatic.
- Can’t be used in non fixating patients.
Advantage
- Screening device
- Easy to use
- No touch technique
- No anesthesia required
27.
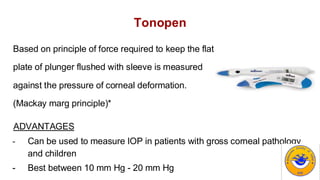
Tonopen
Based on principleof force required to keep the flat
plate of plunger flushed with sleeve is measured
against the pressure of corneal deformation.
(Mackay marg principle)*
ADVANTAGES
- Can be used to measure IOP in patients with gross corneal pathology
and children
- Best between 10 mm Hg - 20 mm Hg
28.
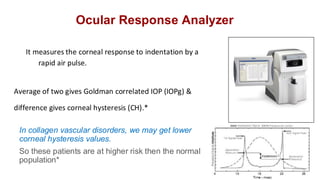
Ocular Response Analyzer
Itmeasures the corneal response to indentation by a
rapid air pulse.
Average of two gives Goldman correlated IOP (IOPg) &
difference gives corneal hysteresis (CH).*
In collagen vascular disorders, we may get lower
corneal hysteresis values.
So these patients are at higher risk then the normal
population*
29.
Corneal Hysteresis (CH)
Cornealhysteresis tells about corneal capacity to absorb & dissipate energy
and it measures the corneal viscoelastic properties. It is a dynamic property,
may change with IOP lowering and stage of disease.
●Normal Values: 9-11
●Low values for CH < 9
●Low values can be associated to a thin cornea or a high IOP.
●Lower CH is associated to a more advanced glaucoma, lower VFI
●NTG patients may have lower CH values
30.
Advantage
- Less influencedby CCT/Corneal biomechanics
- More accurate in patients post corneal refractive surgery
- Also measures Ocular Pulse amplitude- Variation in pressure that occurs
with cardiac cycle.
31.
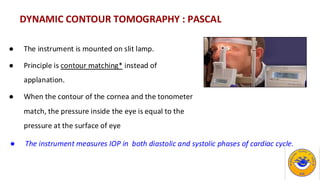
DYNAMIC CONTOUR TOMOGRAPHY: PASCAL
● The instrument is mounted on slit lamp.
● Principle is contour matching* instead of
applanation.
● When the contour of the cornea and the tonometer
match, the pressure inside the eye is equal to the
pressure at the surface of eye
● The instrument measures IOP in both diastolic and systolic phases of cardiac cycle.
32.
Rebound Tonometer
Main objective- Like Blood sugar and BP Monitoring, IOP monitoring can also be
done
- Normal Tension glaucoma
- High risk glaucoma surgeries like One eyed
Trabeculectomy, Non Valved implants where
hypotony can be disastrous
- Monitoring response to new therapy
Indication
33.
Sensimed Triggerfish
- ContinuousIOP monitoring
- The changes in the IOP would cause
change in the circumference of the
cornea
- It uses a soft hydrophilic single use
silicon contact lens, to monitor
fluctuations in diameter of the corneo-
scleral junction.
34.
Transpalpebral tonometer
Measure IOPthrough the eyelids.
- Value in approximating IOP when ordinary tonometry is
not possible, such as with corneal prostheses and totally
scarred corneas
- Examples- Diaton & Proview Phosphene tonometer (1998).
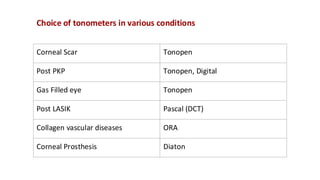
Choice of tonometersin various conditions
Corneal Scar Tonopen
Post PKP Tonopen, Digital
Gas Filled eye Tonopen
Post LASIK Pascal (DCT)
Collagen vascular diseases ORA
Corneal Prosthesis Diaton
38.
Role of tonometryin Glaucoma
Central corneal thickness (CCT) has a direct influence on iOP measurements.
- OHTS for the first time told role of CCT in glaucoma*
- For 40 micron decrease in CCT, the relative risk is 1.71
39.
Q1. In whichpatients CCT should be taken into account
Ans: All the patients
- Glaucoma
- NTG
- Ocular Hypertension
- Post Refractive Surgery
40.
Optimal way
- Ultrasoundbased pachymetry
(Atleast 2 hours after the patient has awakened)
Other ways
- Pentacam/Orbscan
- Specular Microscopy
- Anterior segment OCT
(Mention how you had taken the CCT)
41.
Correction factor
No worldwideagreed nomogram
- 2.5 mm for every 50 micron
- 3.57 mm Hg for 50 micron (Ehler and Hansen)
- 3.3 mm Hg per 50 micron (Doughty)
It is recommended IOP and CCT to be recorded separately and no
correction factor
42.
Clinical Implications
- Lowercorneal thickness is very strong indicator to look for progression
- Though thicker corneas are definitely give a higher IOP, Still even these
patients need a very careful follow up
- In refractive surgery it would cause a major shift, so IOP recording can
fluctuate a lot so very careful ONH assessment is needed