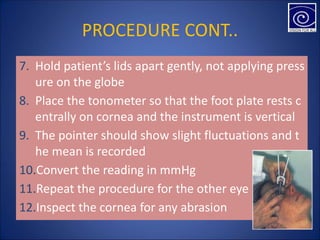
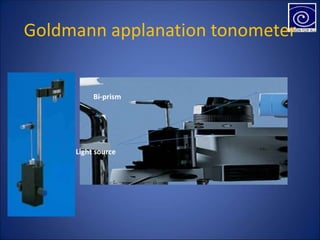
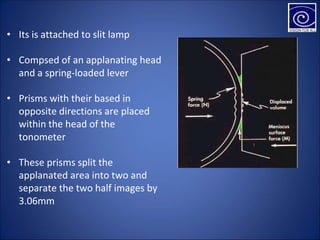
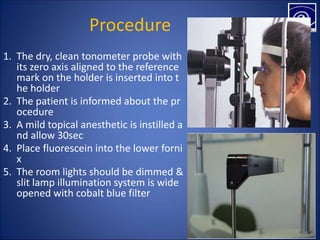
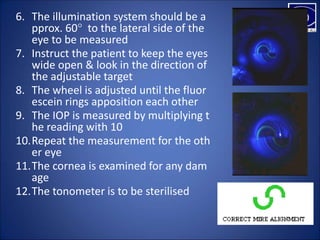
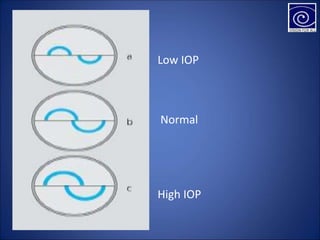
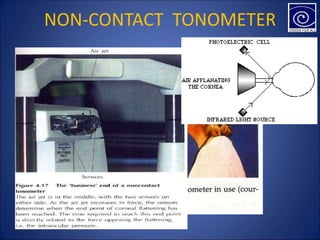
This document discusses different types of tonometers used to measure intraocular pressure. It describes indentation tonometers like the Schiotz tonometer which measures indentation depth from a known weight. Applanation tonometers like the Goldmann tonometer flatten a circular area of the cornea to measure pressure. Non-contact tonometers use an air puff to detect inward and outward corneal movement at different pressures. Accuracy can be affected by corneal properties, accommodation, and proper technique.