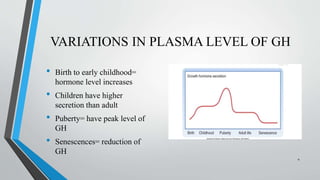
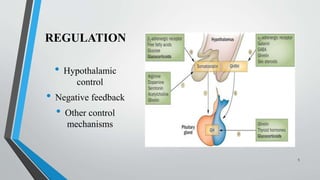
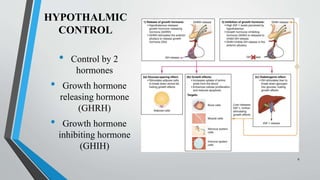
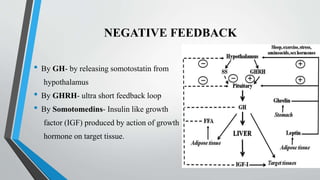
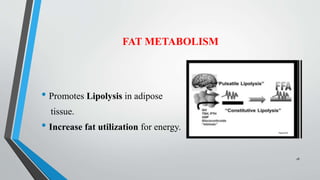
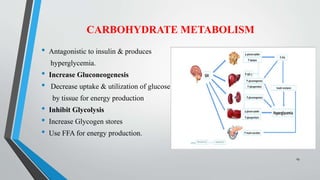
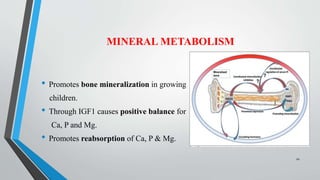
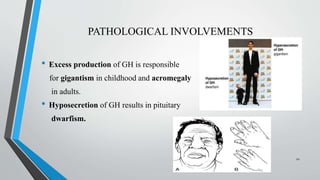
Growth hormone is secreted by the anterior pituitary gland and regulates postnatal growth, protein synthesis, and metabolism. Its secretion is controlled by the hypothalamus through growth hormone-releasing hormone and growth hormone-inhibiting hormone. Growth hormone binds to receptors on target tissues and activates the JAK-STAT pathway to promote growth, increase fat metabolism, and influence protein and carbohydrate metabolism. Abnormal growth hormone secretion can cause gigantism, acromegaly, or dwarfism. Somatostatin and octreotide inhibit growth hormone secretion and are used to treat acromegaly.





















































![establishing_pv_centers_in_industry_AND_NATIONAL_PROGRAMME[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/establishingpvcentersinindustryandnationalprogramme1-230725101256-d16cc241-thumbnail.jpg?width=640&height=640&fit=bounds)

































