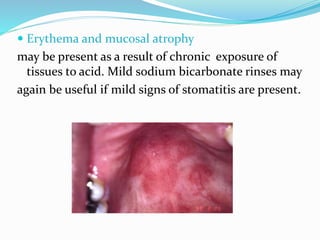
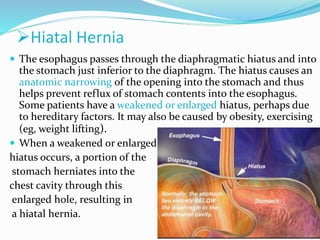
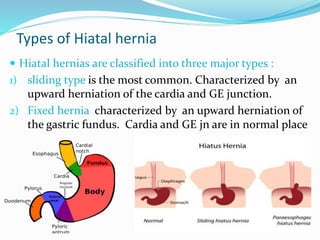
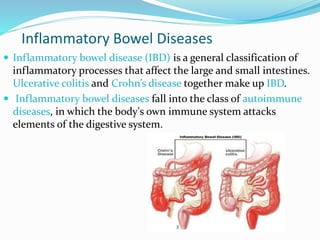
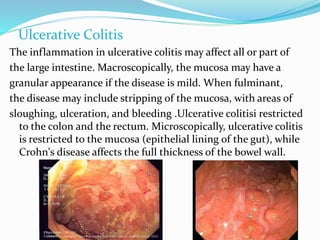
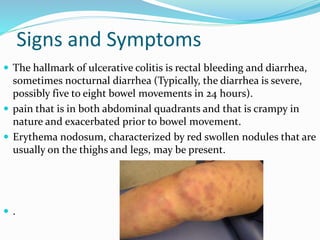
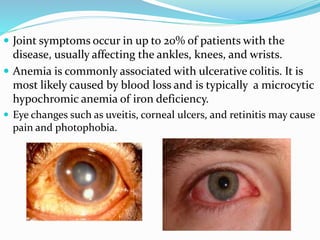
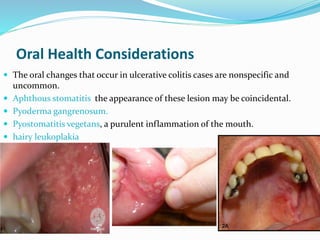
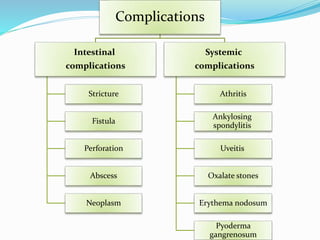
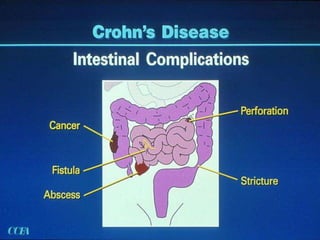
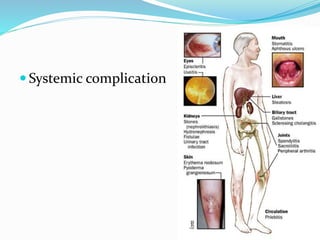
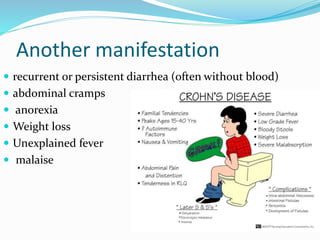
The document discusses diseases of the upper and lower digestive tract. The upper tract includes the esophagus, stomach, and duodenum. Gastroesophageal reflux disease (GERD) and hiatal hernia are common upper tract diseases described. In the lower tract, duodenal ulcers, inflammatory bowel diseases like ulcerative colitis and Crohn's disease, and their signs, symptoms, and oral health considerations are outlined. Crohn's can involve any GI part and cause complications like strictures, while ulcerative colitis only impacts the colon.