Downloaded 1,140 times


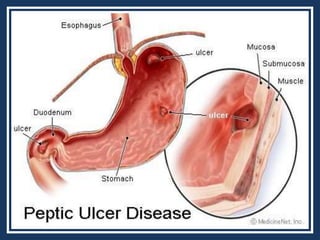

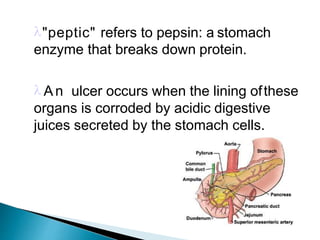
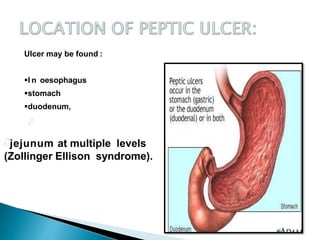
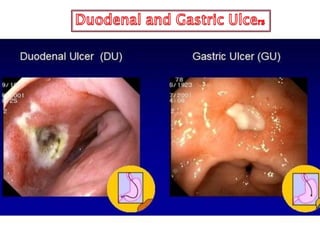
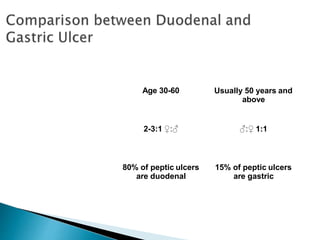
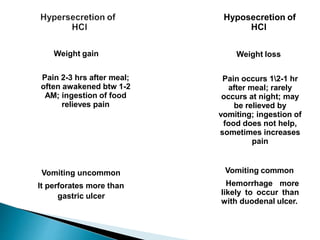
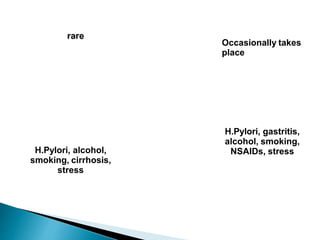
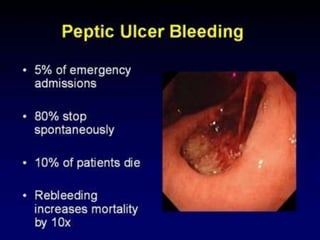
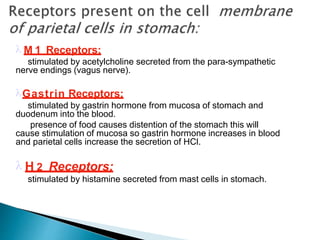
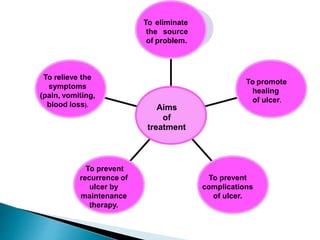
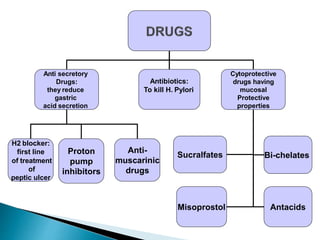
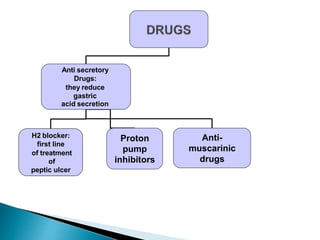
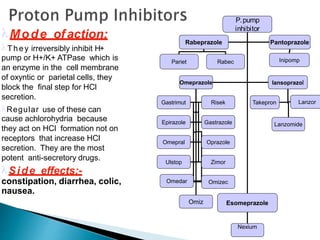


This document provides information about peptic ulcers, including their causes, symptoms, diagnosis, and treatment. Peptic ulcers occur when the lining of the stomach, duodenum, or esophagus is corroded by acidic digestive juices. Common causes are infection with H. pylori bacteria and long-term use of NSAIDs. Symptoms vary depending on the location of the ulcer but can include abdominal pain, nausea, vomiting, weight loss, and fatigue. Diagnosis involves blood, breath, stool, or biopsy tests to detect H. pylori. Treatment aims to relieve symptoms, promote healing, and prevent complications and recurrence. It involves use of medications to reduce acid secretion such as PPIs, H









































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)













