Downloaded 76 times
![Time of DeathTime of Death
Can estimate time of death from
• body temperature (algor mortis)
estimate: [98.6 o
F – rectal temp]/1.5
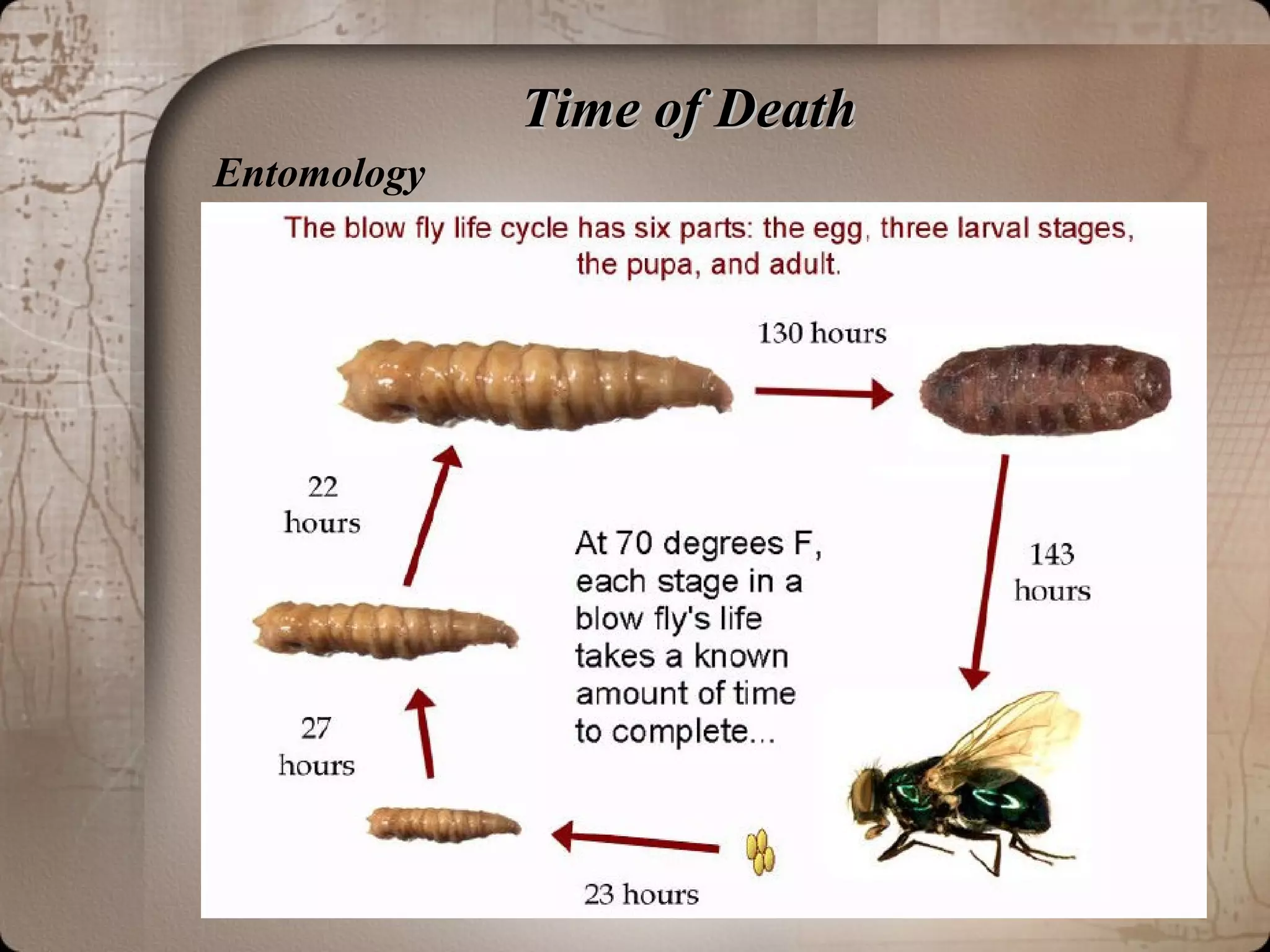
• insect action (forensic entomology)
• stomach contents (stage of digestion)
• last known activity (last sighting, newspaper/mail)
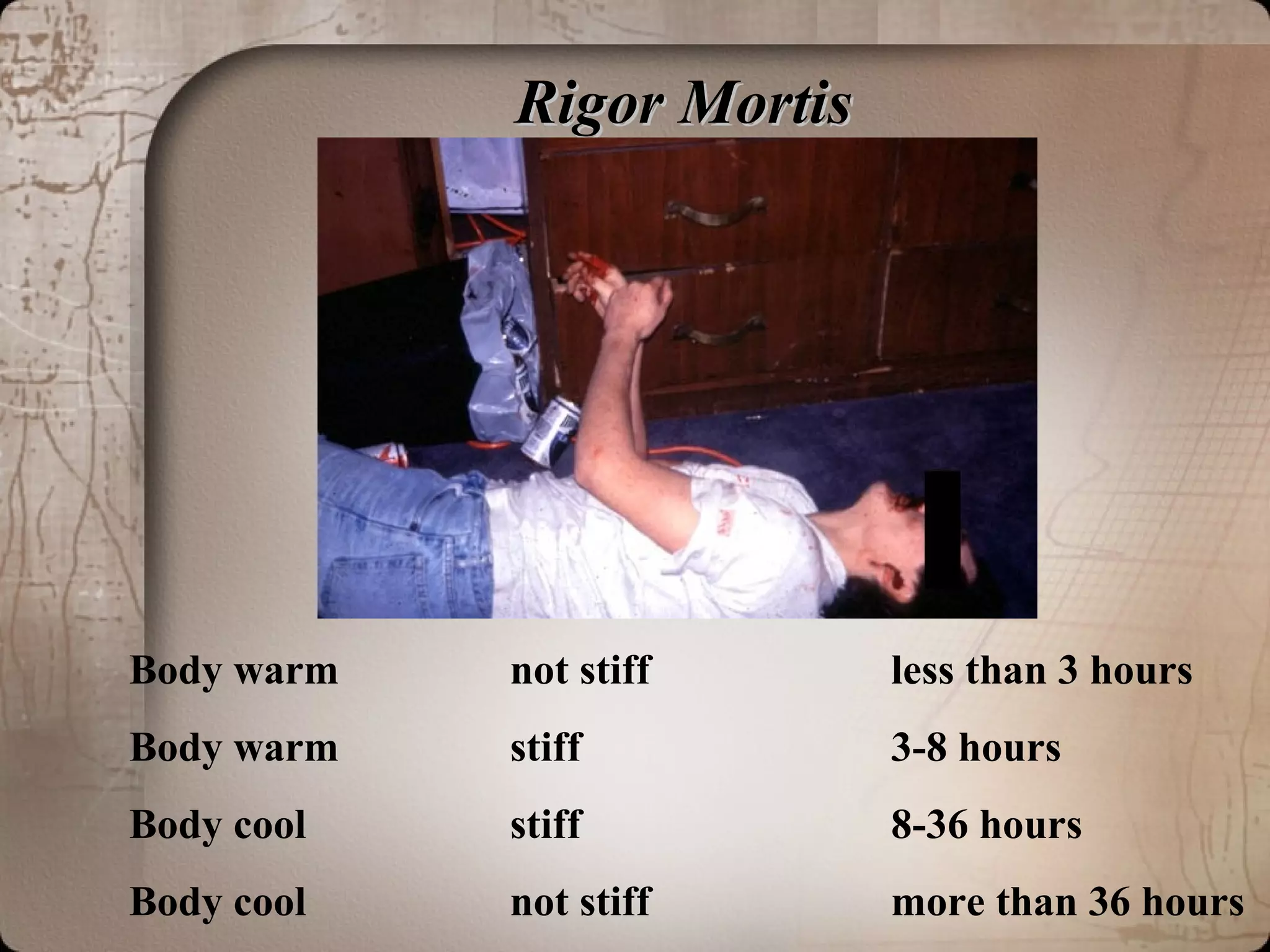
• normal postmortem changes](https://image.slidesharecdn.com/forensicpathologynotesby-dr-150307131419-conversion-gate01/75/Forensic-pathology-notes-by-dr-armaan-singh-3-2048.jpg)
![Time of DeathTime of Death
Can estimate time of death from
• body temperature (algor mortis)
estimate: [98.6 o
F – rectal temp]/1.5
• insect action (forensic entomology)
• stomach contents (stage of digestion)
• last known activity (last sighting, newspaper/mail)
• normal postmortem changes](https://image.slidesharecdn.com/forensicpathologynotesby-dr-150307131419-conversion-gate01/75/Forensic-pathology-notes-by-dr-armaan-singh-5-2048.jpg)



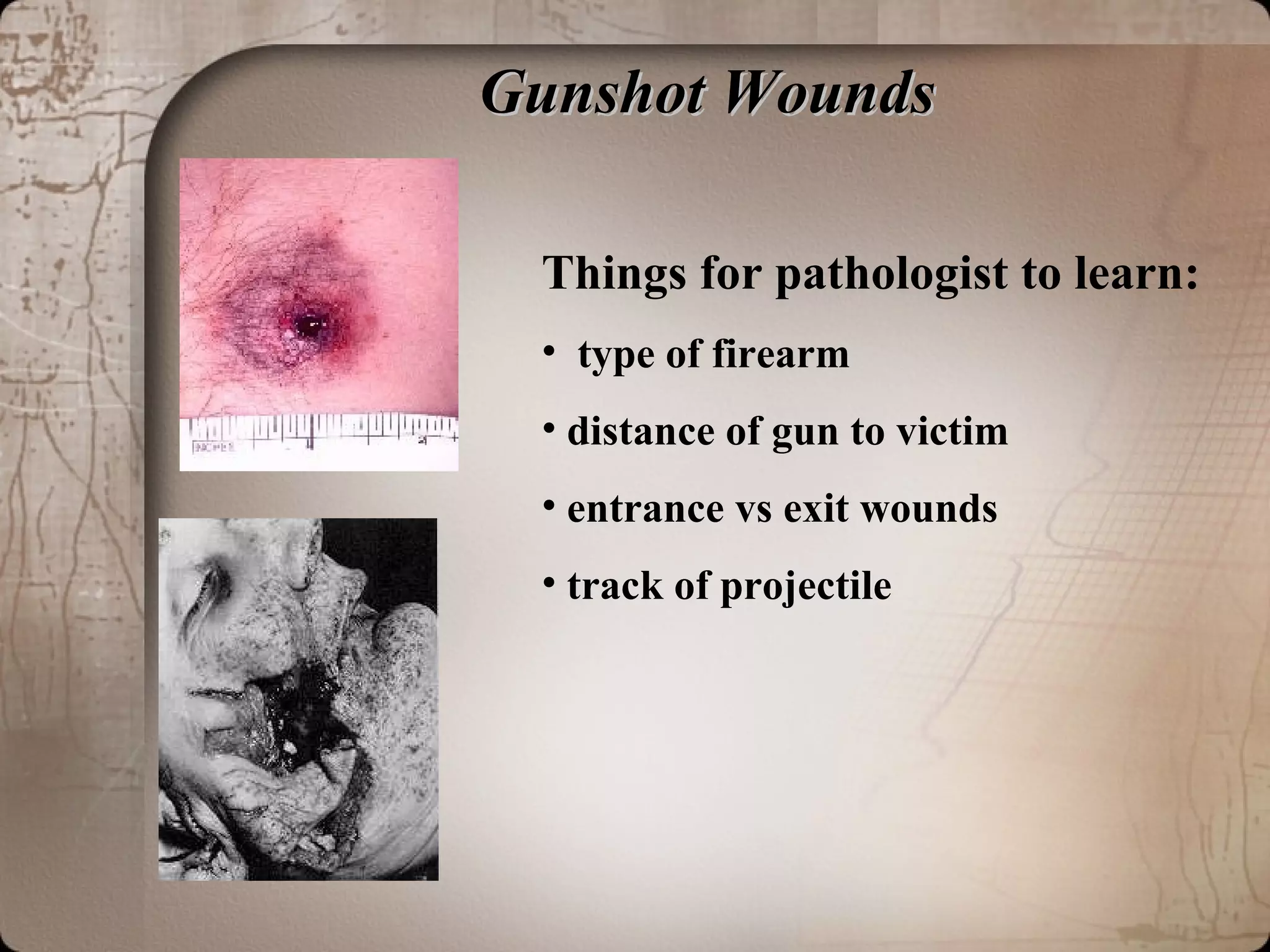
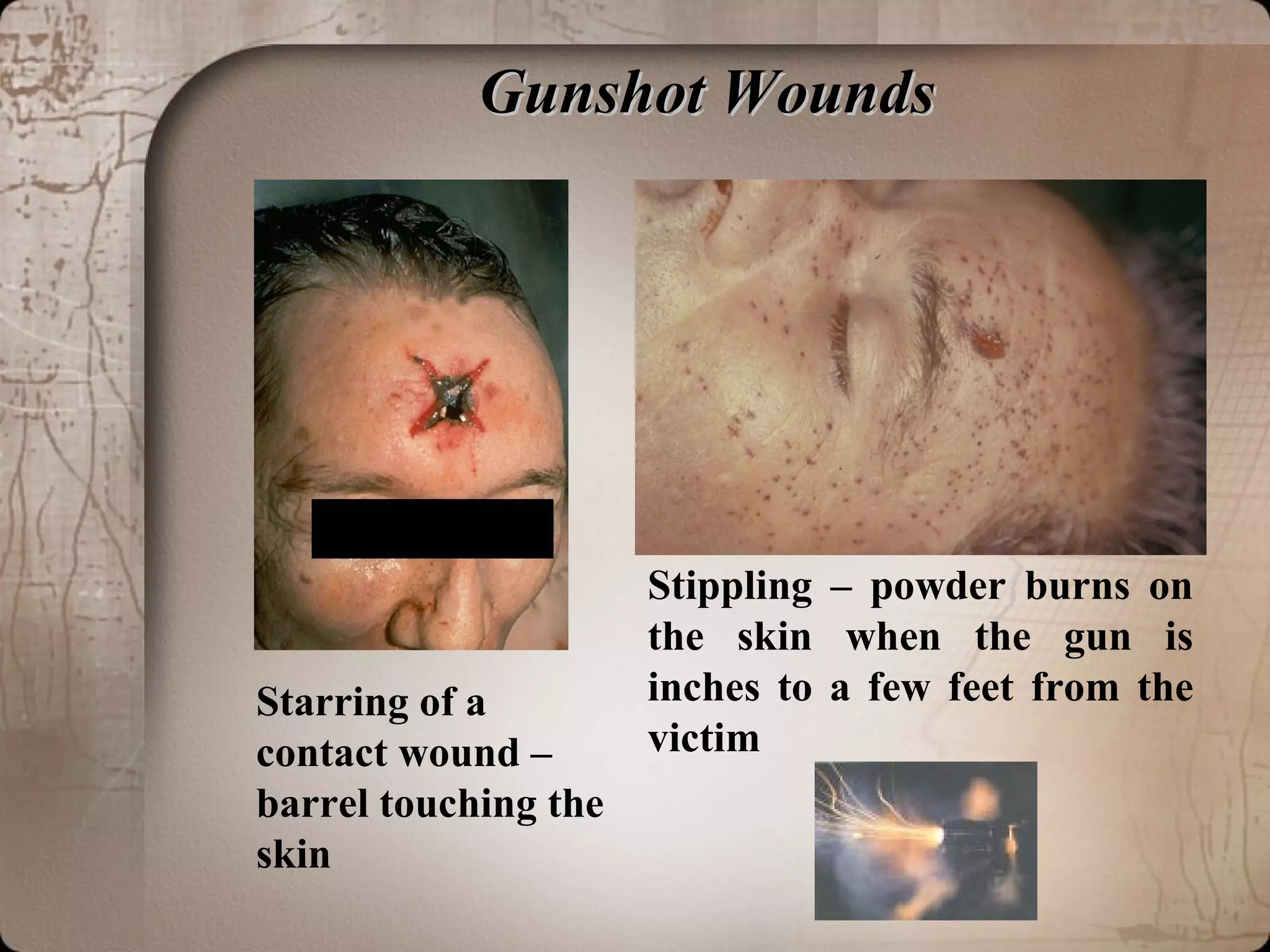
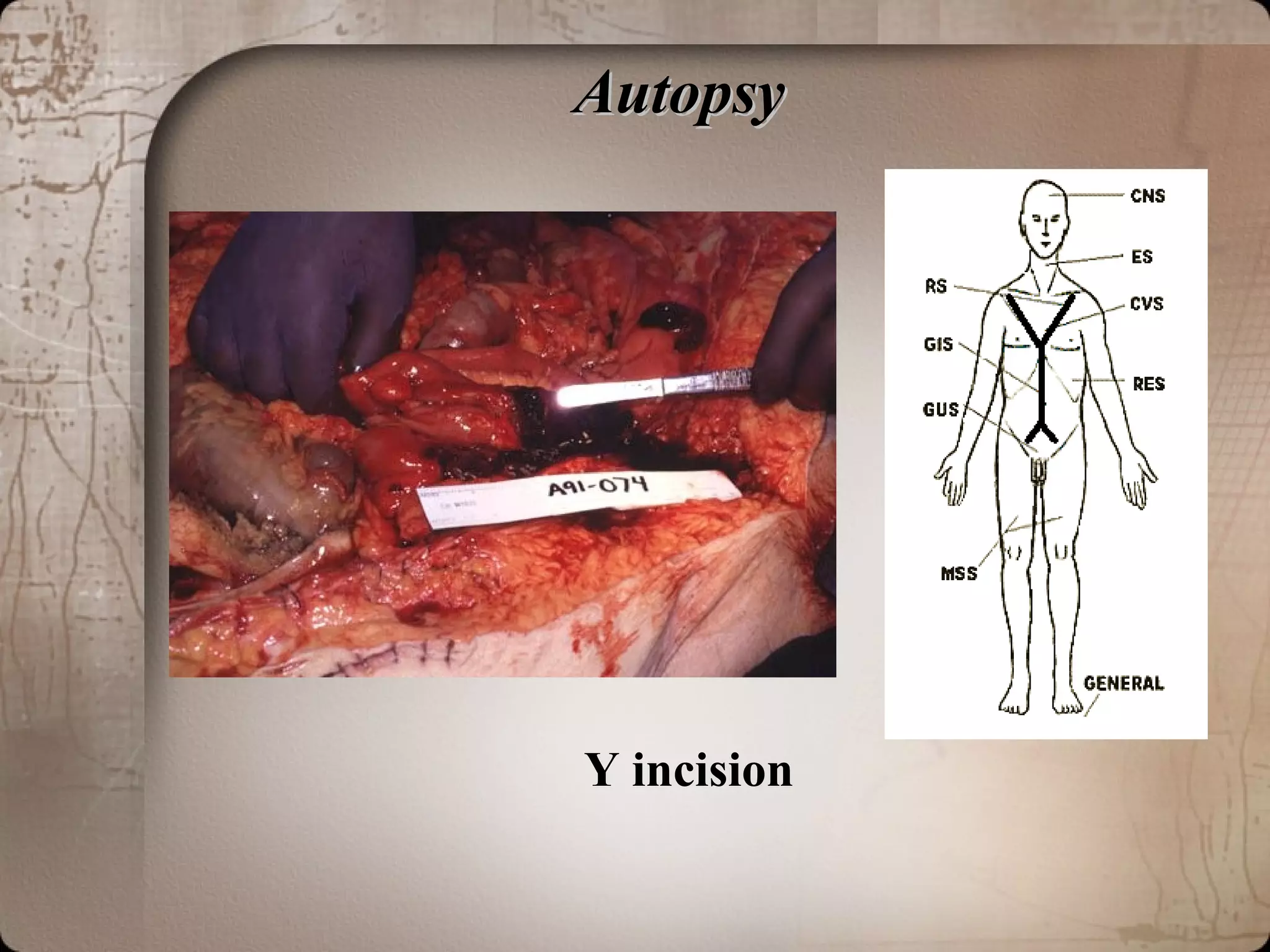
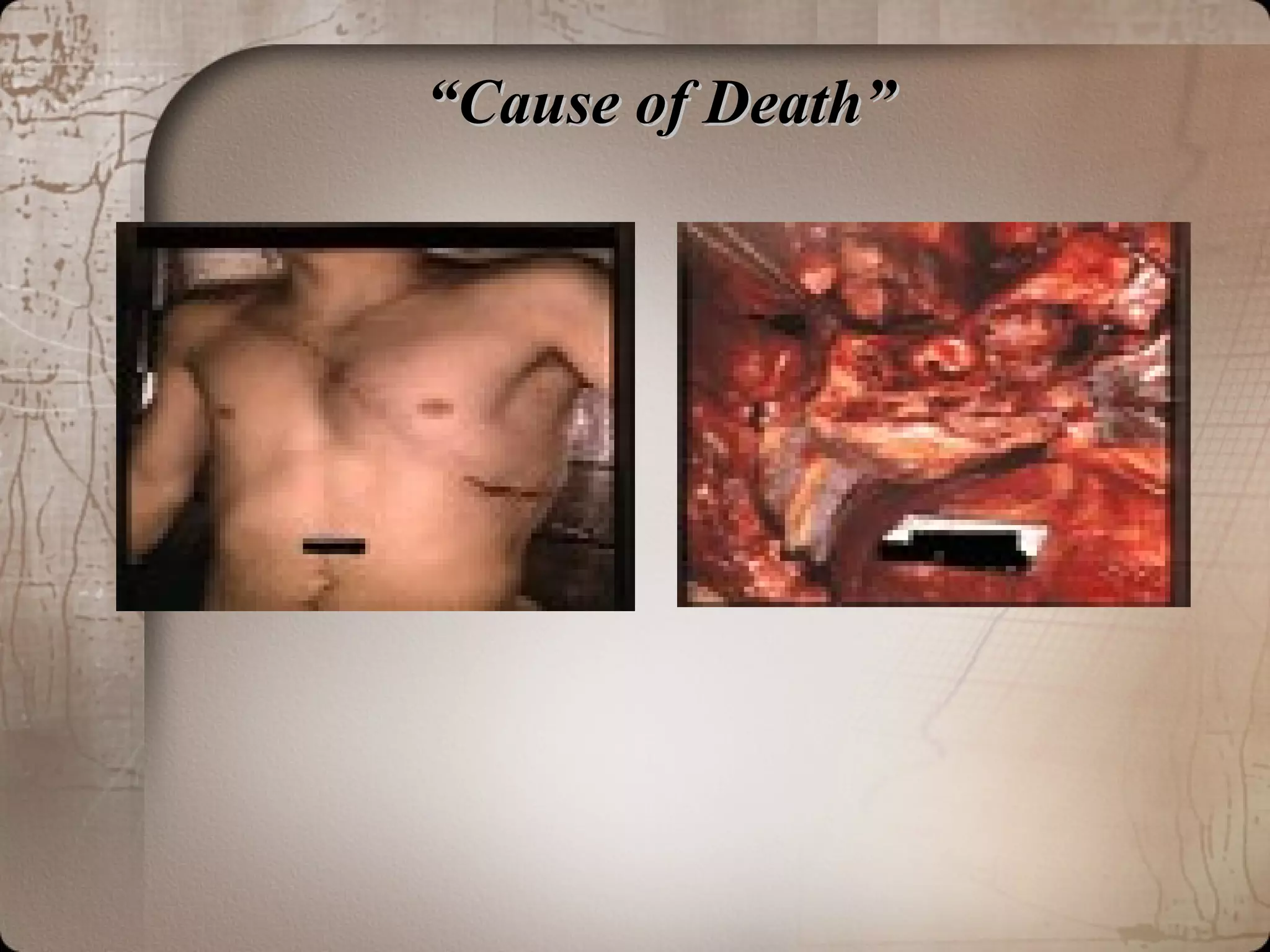

The document discusses forensic pathology and autopsy procedures. It describes the role of the forensic pathologist as determining the cause, manner, and time of death through postmortem examination. It outlines the typical steps of an autopsy, including external examination, a Y-shaped incision, examination of organs, and analysis of trauma wounds or other signs that could indicate the cause of death. Key autopsy goals are to examine the body for injuries or diseases that may have led to death.











































































































