Downloaded 90 times

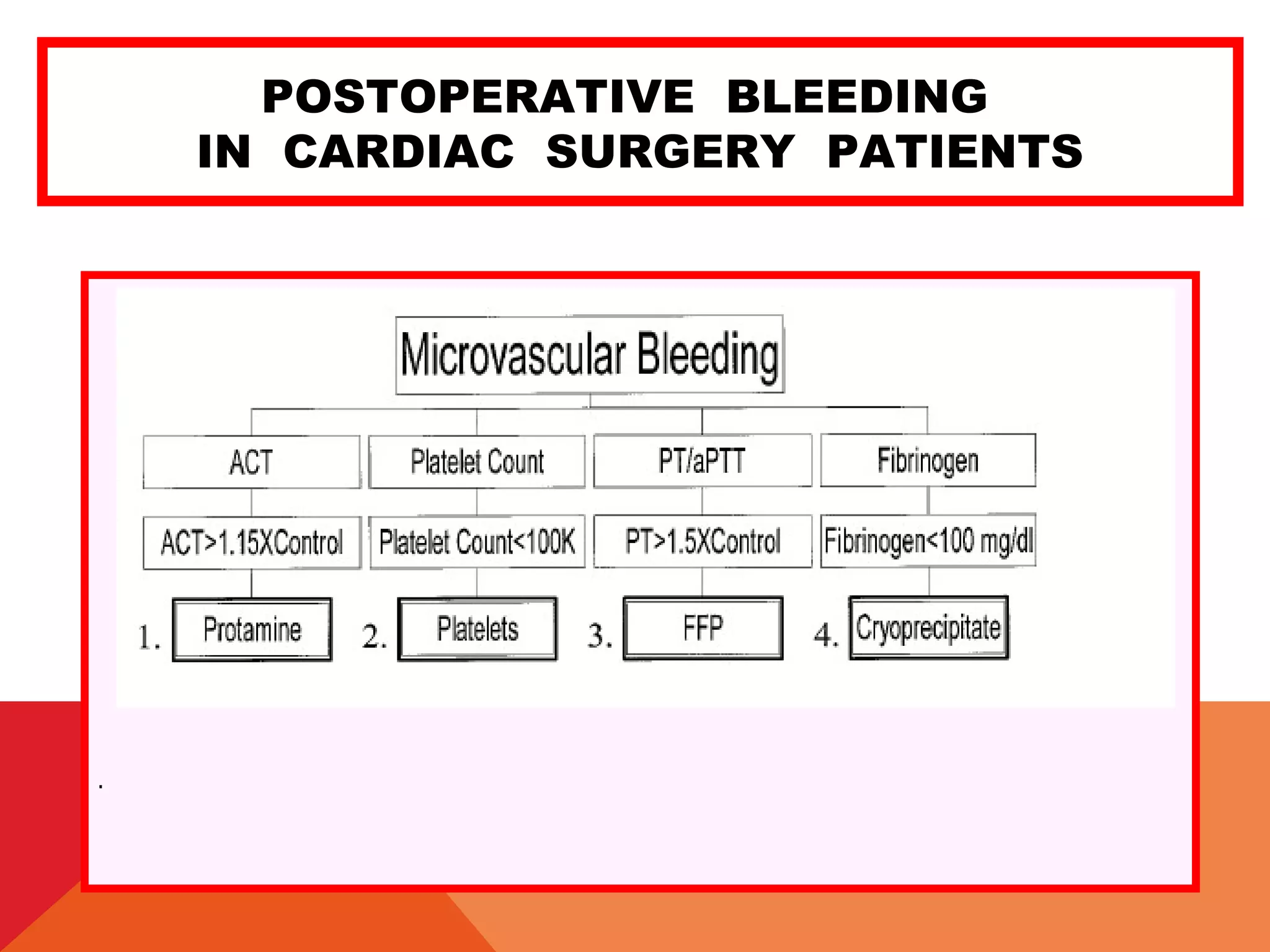

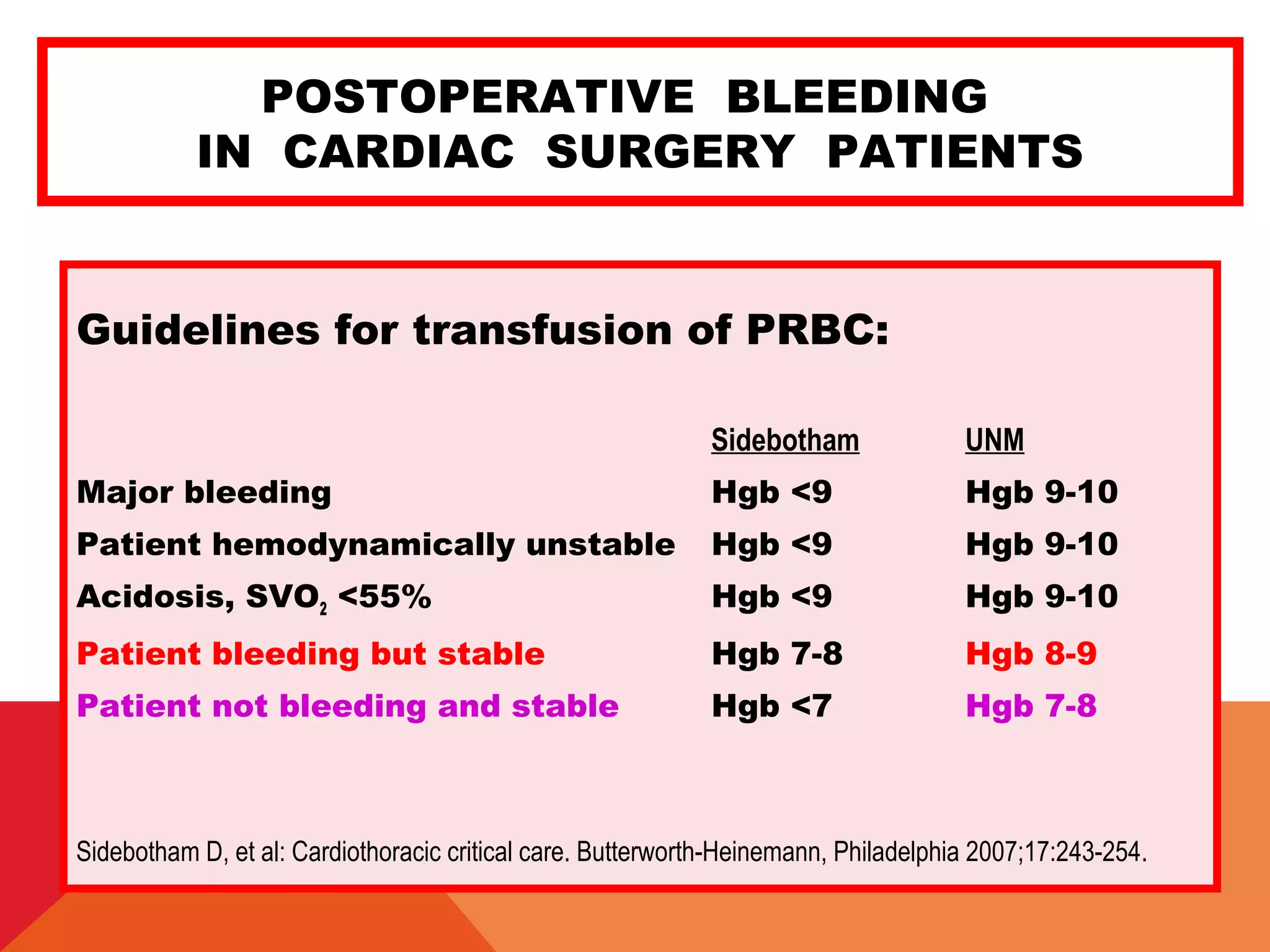
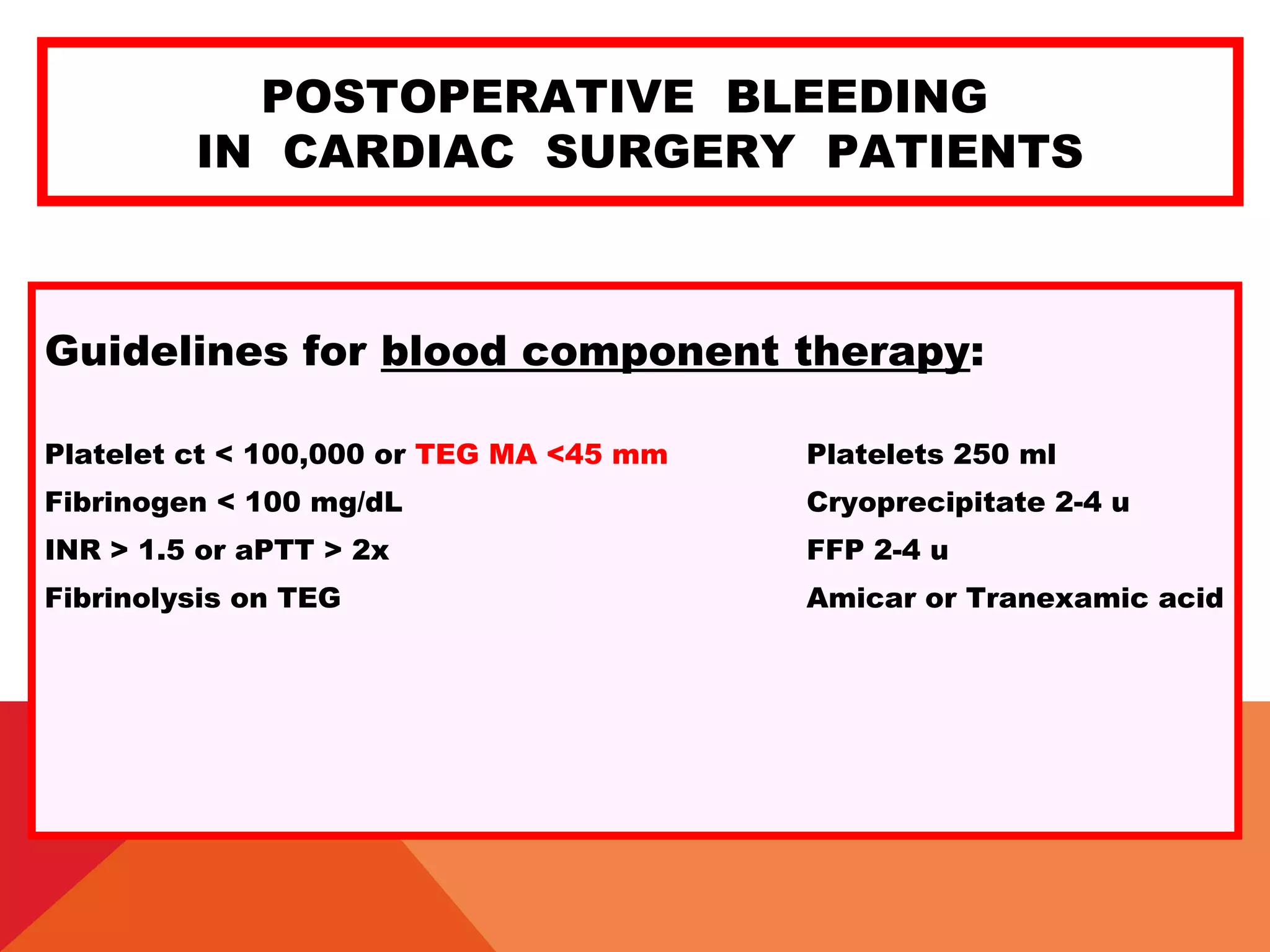
![POSTOPERATIVE BLEEDING
IN CARDIAC SURGERY PATIENTS
Coagulation factors:
Fibrinogen concentrate (RiaSTAP 1300 mg/50 ml) 70 mg/kg (will ↑ fibr 120
mg/dL)
Recombinant Factor VIIa (NovoSeven) 50 mcg/kg (1-2% TE complic)
90 mcg/kg (4%TE complic)
Prothrombin Complex Concentrates
(Bebulin VH) [factors II,IX,X] 70-95 units/kg
(Beriplex P/N) [factors II,VII,IX,X] 25-50 units/kg](https://image.slidesharecdn.com/postoperativebleedingguidelinesfortransfusion-150304121653-conversion-gate01/75/Postoperative-bleeding-guidelines-for-transfusion-23-2048.jpg)

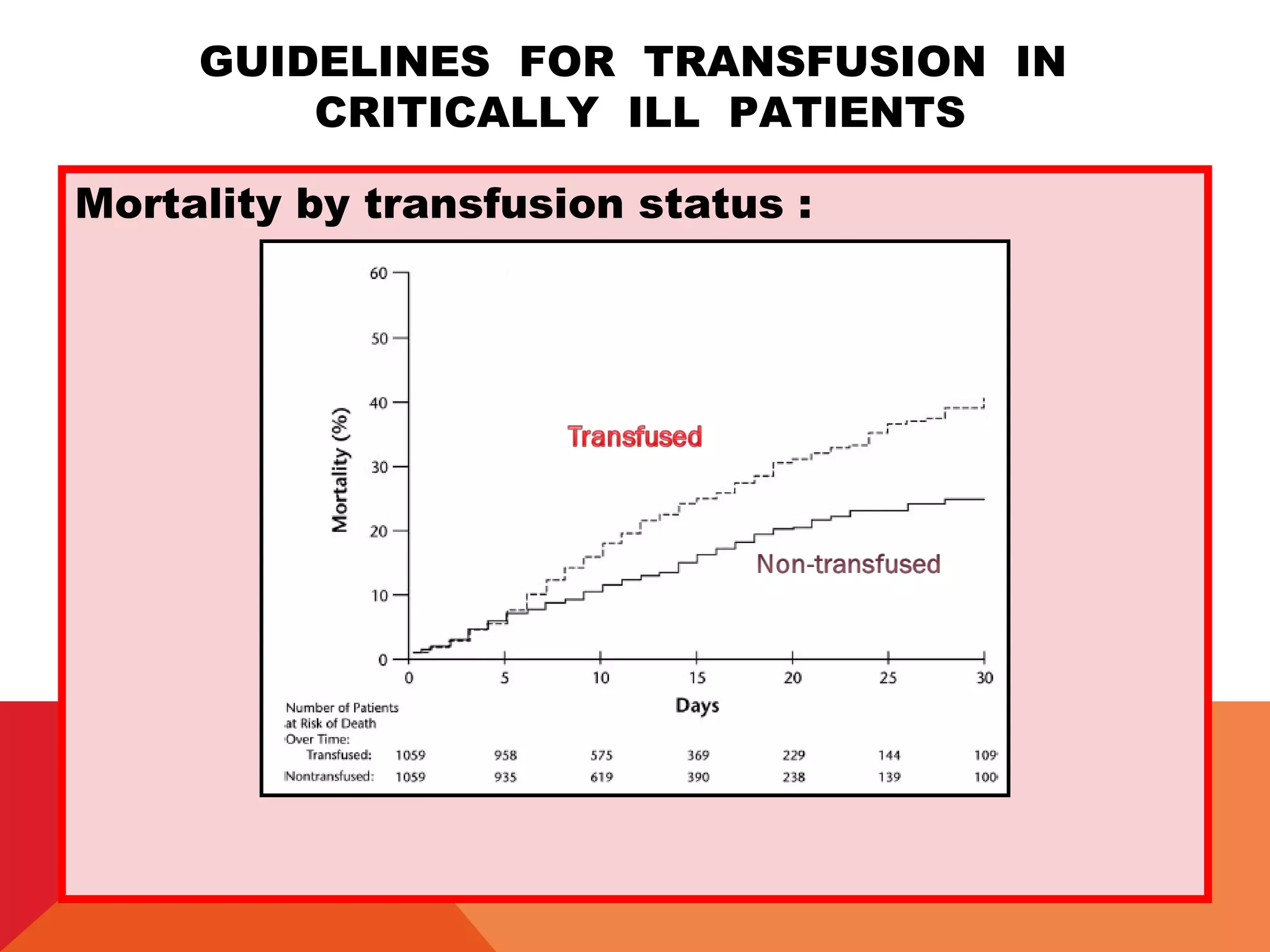
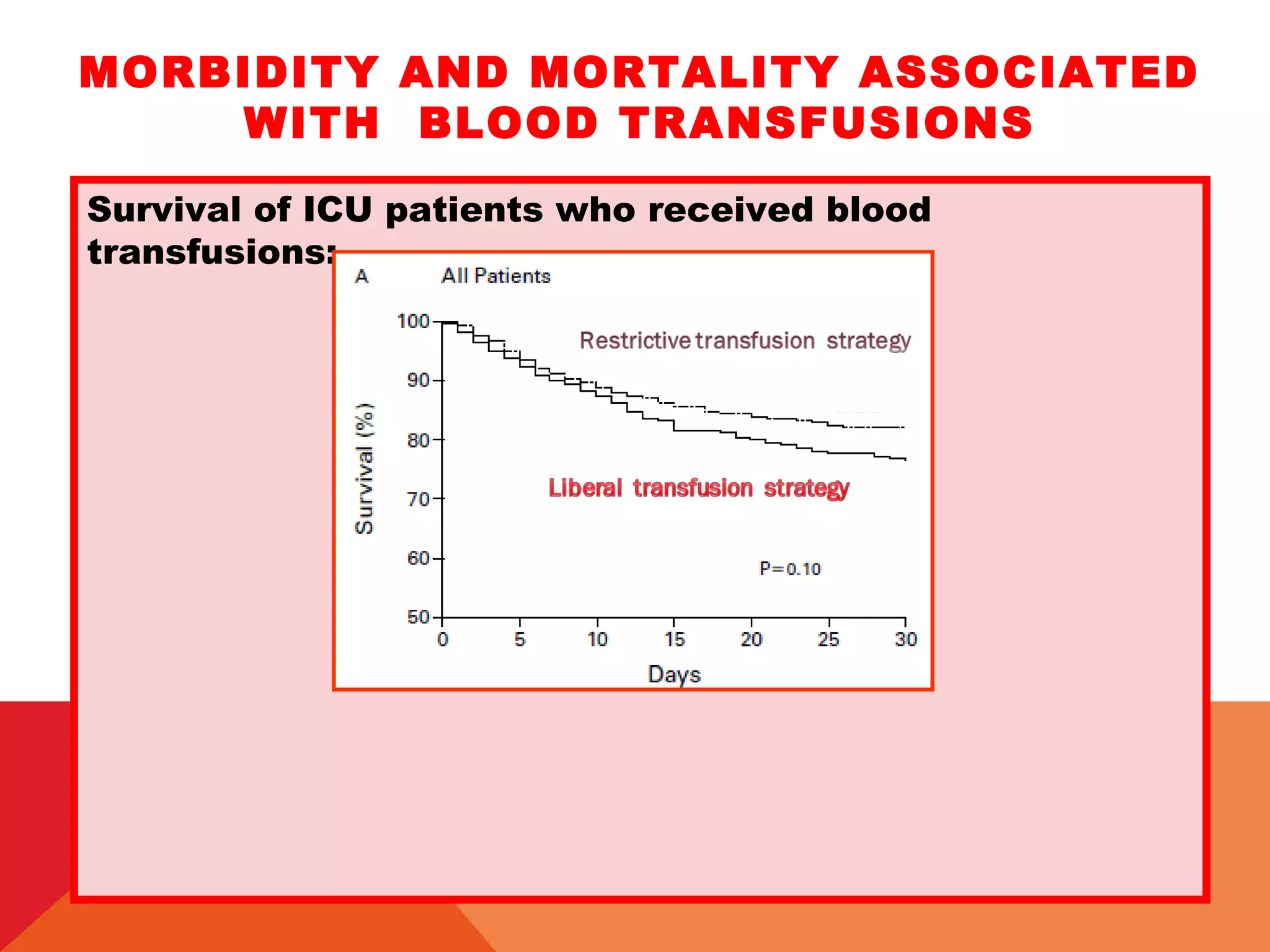
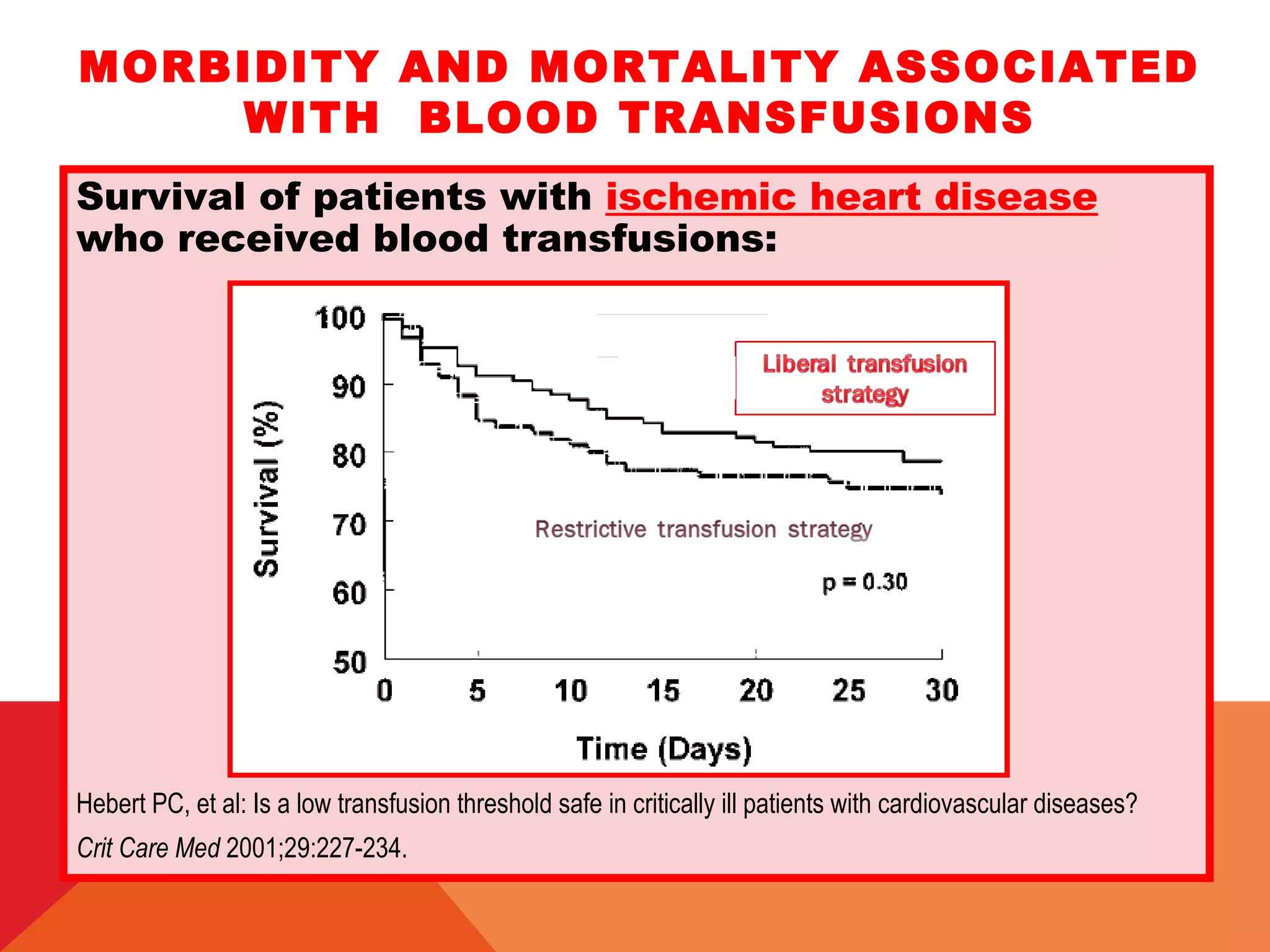
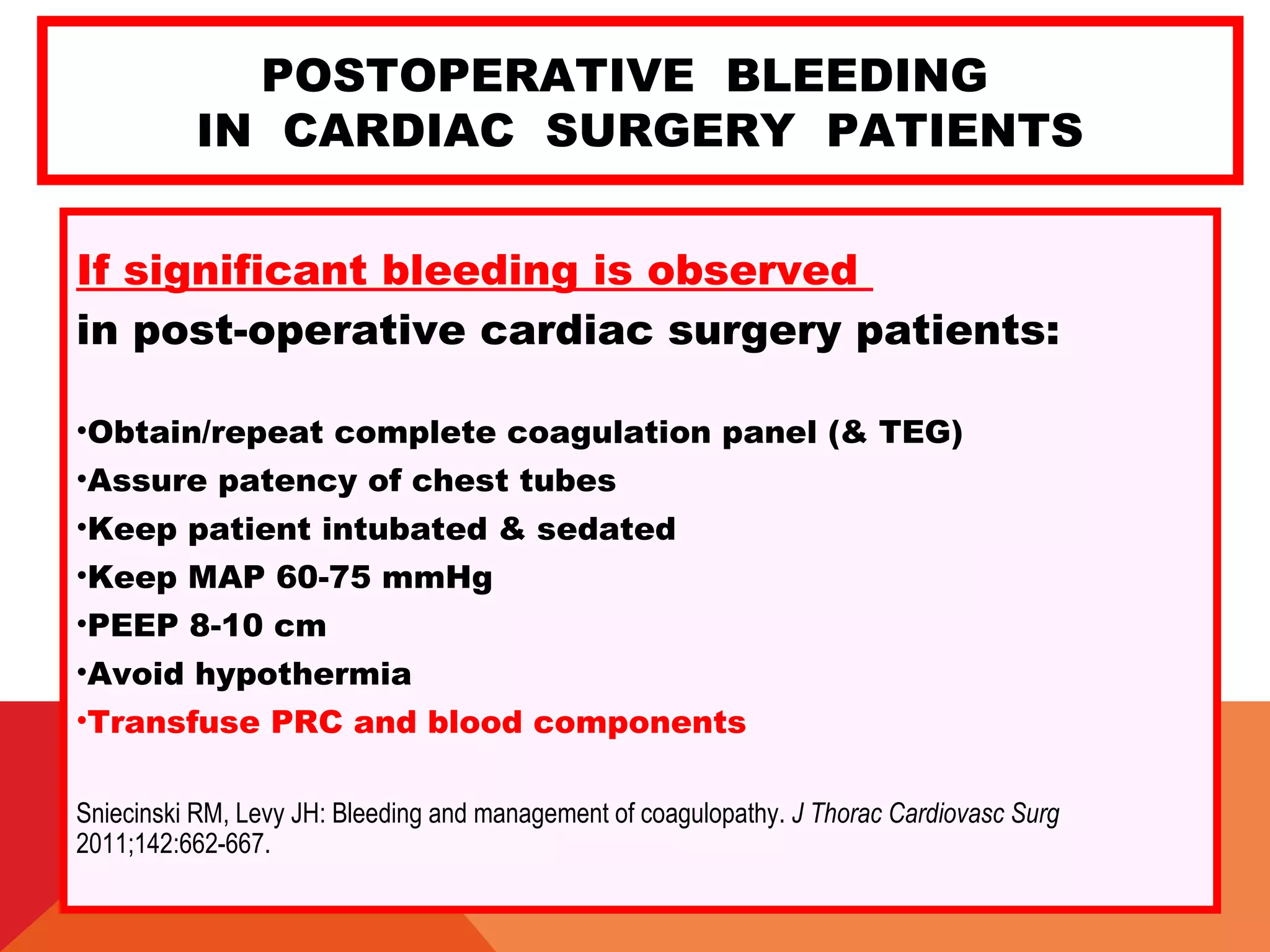
This document discusses guidelines for transfusion therapy and management of postoperative bleeding in cardiac surgery patients. It provides an overview of factors that can influence bleeding, complications of blood transfusions, and tests to assess coagulation status. The document outlines guidelines for transfusion of blood products like platelets, plasma, cryoprecipitate based on results of coagulation tests or thromboelastography. It also provides guidelines for surgical re-exploration based on chest tube output. Management of massive bleeding and tamponade is discussed.