Downloaded 34 times
![MANAGEMENT OF LEFT HEART FAILURE WITH
SECONDARY PULMONARY HYPERTENSION
IN CARDIAC SURGERY PATIENTS
Nesiritide (Natrecor):
• Standard Dilution:
[1.5 mg] [250 ml D5W, D5½S or NS]
• Loading dose:
2 mcg/kg over 20 min
• Followed by 0.01 mcg/kg/min
• Continuous infusion x 48 hours](https://image.slidesharecdn.com/postoperativepulmonaryhypertension-150304033251-conversion-gate01/85/Postoperative-pulmonary-hypertension-9-320.jpg)
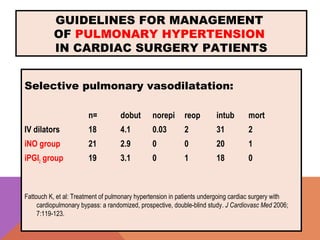
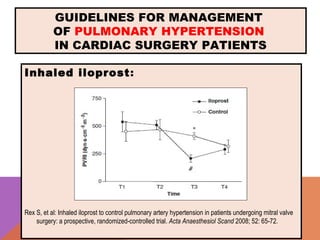
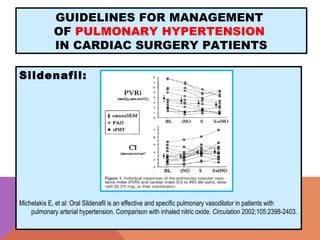
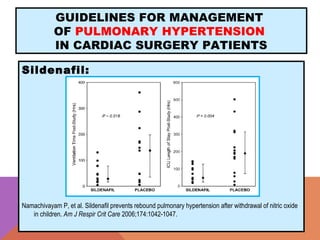

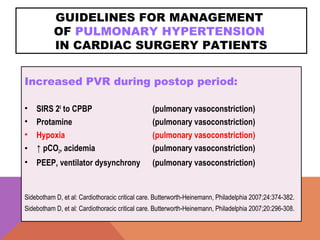
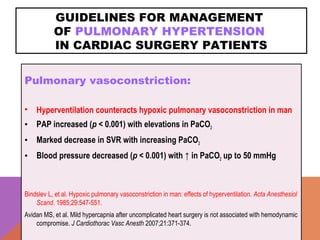
The document provides guidelines for the management of pulmonary hypertension in cardiac surgery patients. It discusses causes of increased pulmonary vascular resistance postoperatively including hypoxia, hypercarbia, acidosis, and pulmonary vasoconstriction. It recommends treating the underlying cause by avoiding factors that cause pulmonary vasoconstriction. For passive pulmonary hypertension, it suggests improving left ventricular contractility and decreasing mitral regurgitation. It also discusses selective pulmonary vasodilators like inhaled nitric oxide, prostacyclin, and iloprost as well as oral sildenafil.