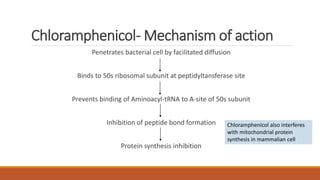
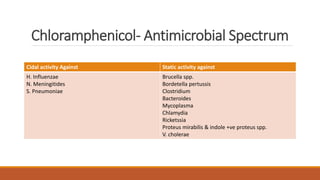
Chloramphenicol is a broad-spectrum antibiotic produced by Streptomyces venezuele that was introduced in 1948. It works by binding to the 50s ribosomal subunit and inhibiting protein synthesis in bacteria. However, it can also interfere with mitochondrial protein synthesis in mammalian cells, causing serious and potentially fatal blood disorders. For this reason, chloramphenicol is now reserved for life-threatening infections like meningitis or rickettsial infections when safer alternatives cannot be used due to resistance or allergies. While effective against a wide range of bacteria, chloramphenicol's use is limited by its risk of toxicities like aplastic anemia and gray baby syndrome in neonates.











![ANTI-TB AND ANTI LEPROTIC DRUGS [MEDICINAL CHEMISTRY] BY P.RAVISANKAR.](https://cdn.slidesharecdn.com/ss_thumbnails/anti-tbdrugs-130615221719-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)


































































