Downloaded 862 times
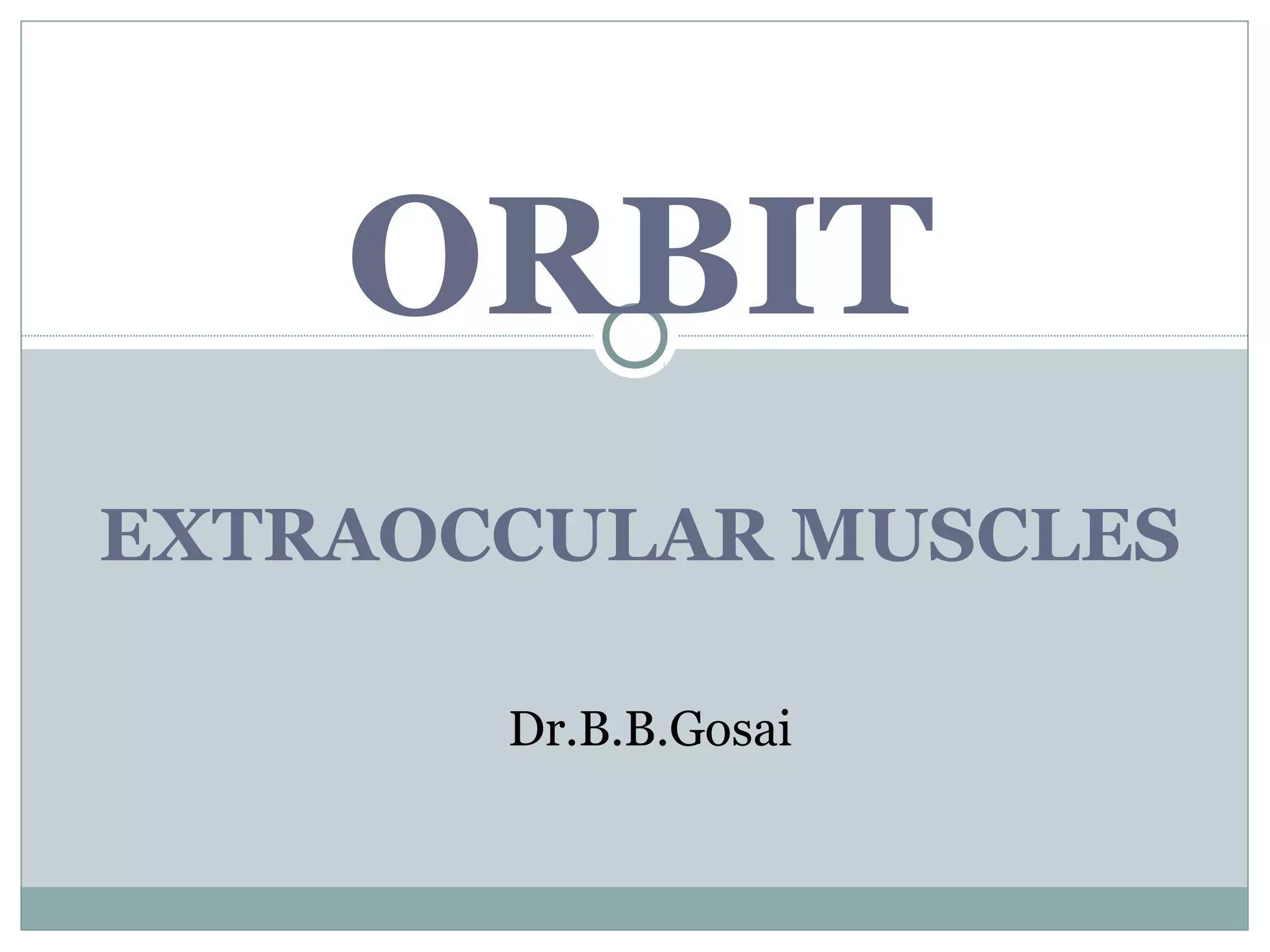
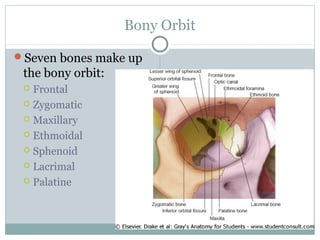
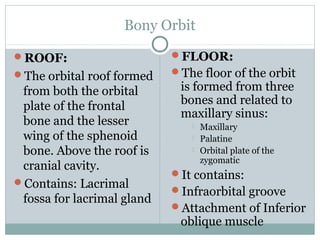
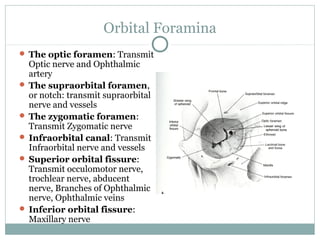
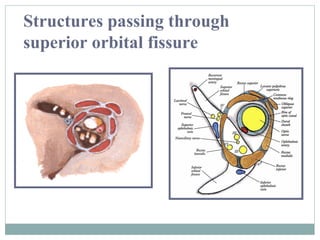
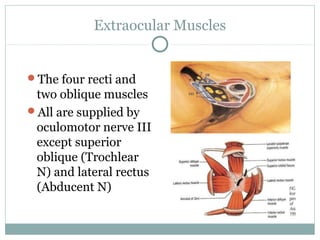
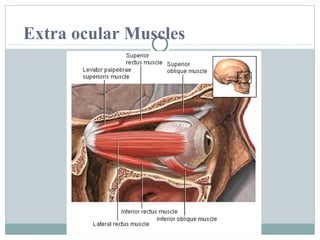
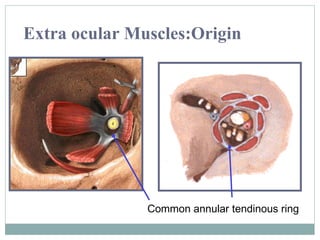
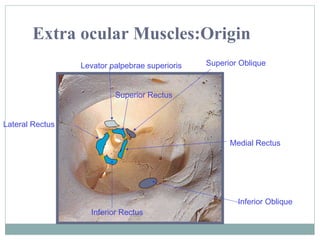
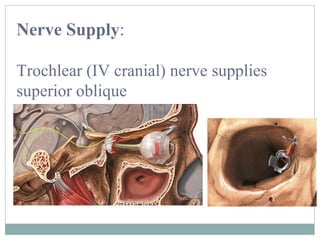
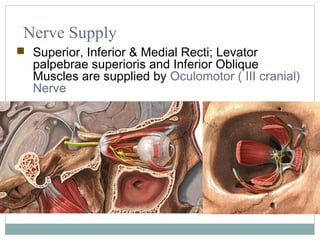
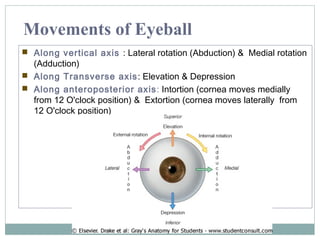
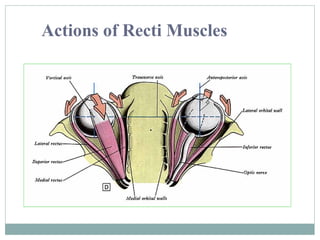
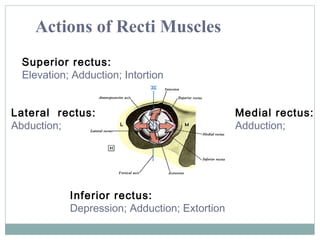
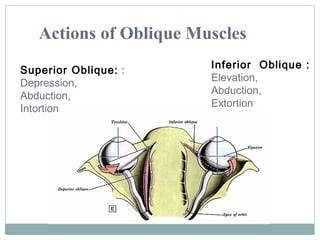
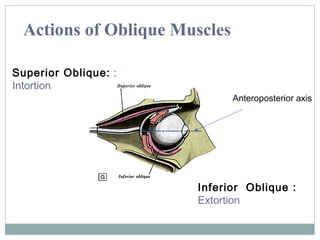
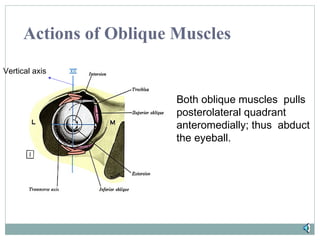
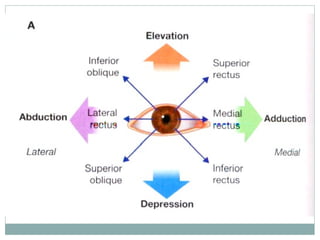
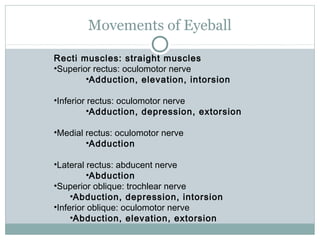
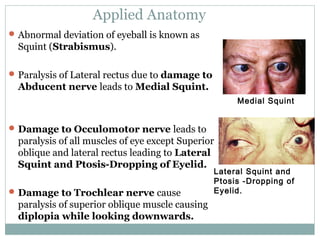
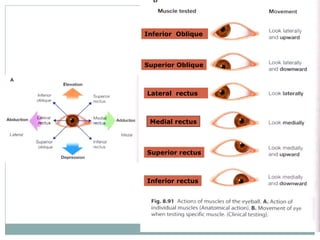
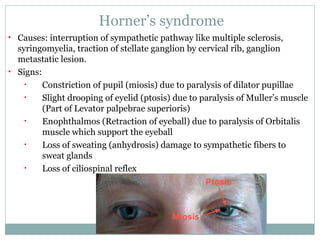

The document describes the anatomy of the bony orbit and the extraocular muscles within. It discusses the seven bones that make up the bony orbit, including the frontal, zygomatic, maxillary, ethmoid, sphenoid, lacrimal and palatine bones. It describes the roof, floor, medial wall and lateral wall of the orbit. It then discusses the extraocular muscles, including the four rectus muscles, two oblique muscles and levator palpebrae superioris. It details the origin, insertion, nerve supply and actions of each muscle. Finally, it discusses some clinical implications like strabismus and Horner's syndrome.























































































