
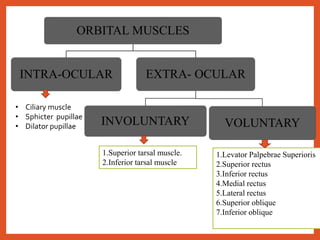
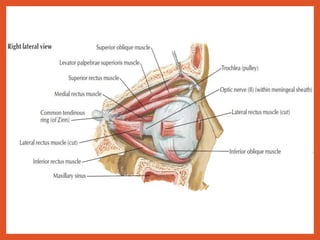
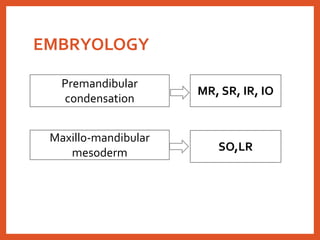


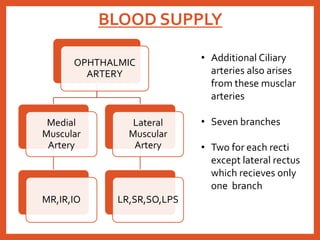




This document provides an overview of orbital and extraocular muscles: 1. It describes the anatomy, embryology, blood supply, nerve supply and actions of the 7 extraocular muscles - superior, inferior, medial and lateral rectus, superior and inferior oblique, and levator palpebrae superioris. 2. Key points about the rectus muscles include their origin, course, insertion locations on the sclera, and primary and secondary actions. 3. The oblique muscles intort and depress or extort and elevate the eyeball respectively as their primary actions. 4. Embryologically, the muscles develop from mesoderm and form a single muscle cone that later separates


















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


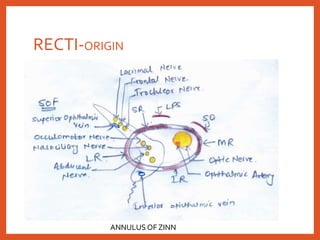
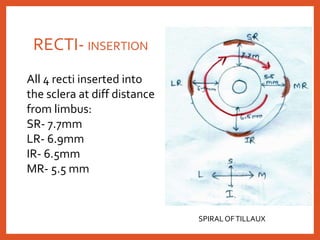
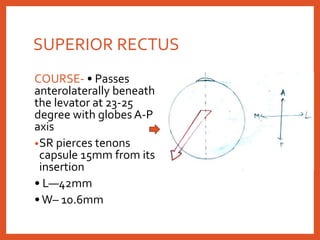
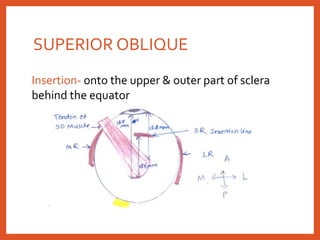
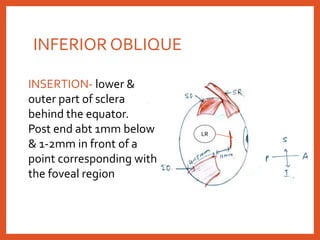
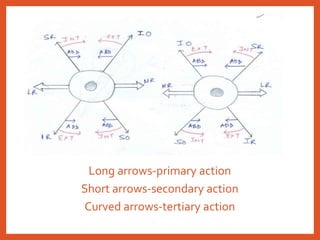
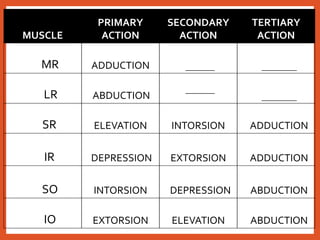
![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

