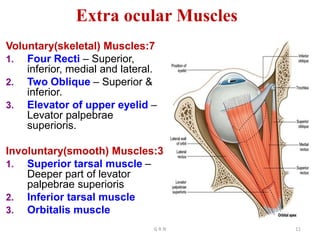
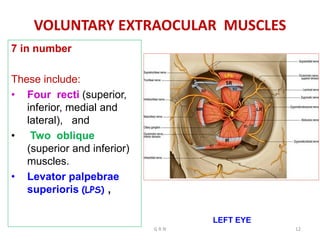
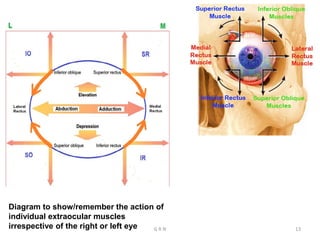
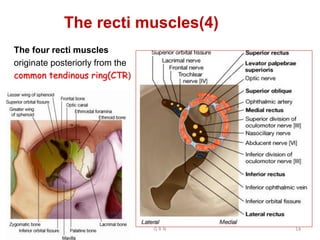
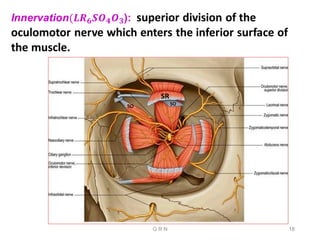
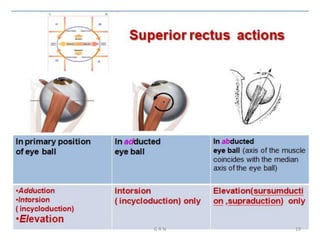
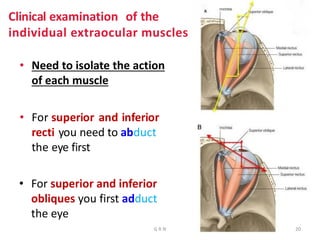
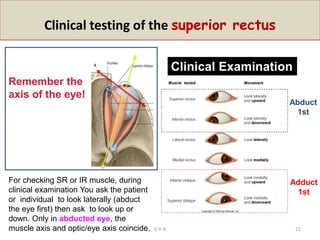
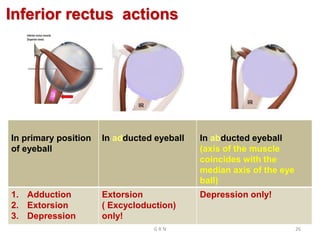
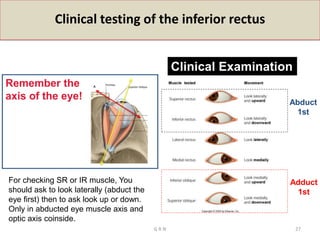
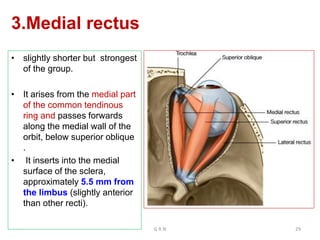
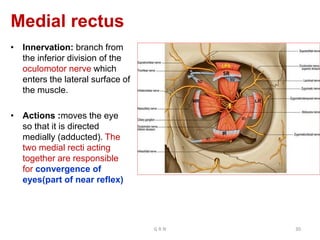
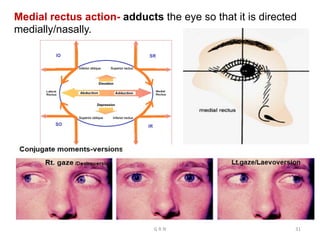
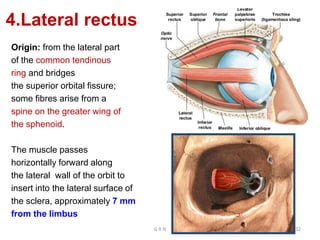
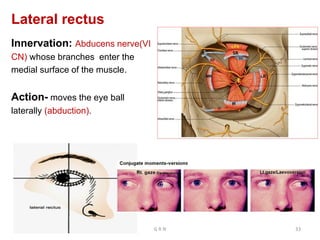
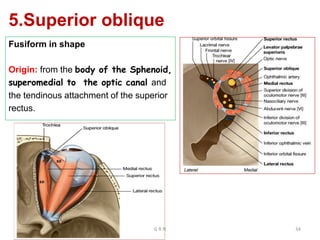
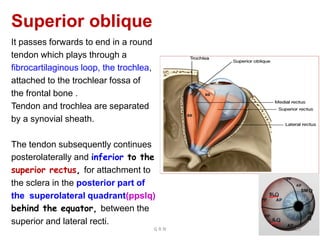
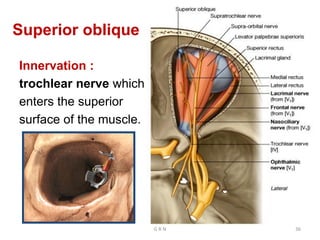
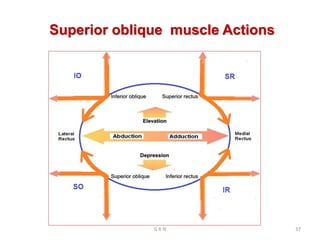
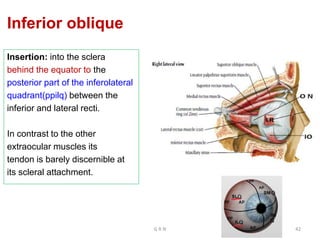
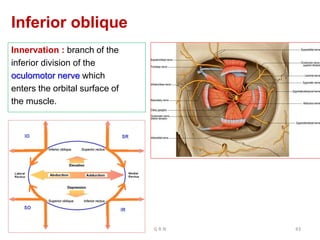
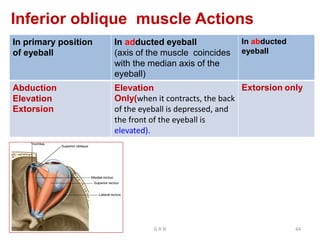
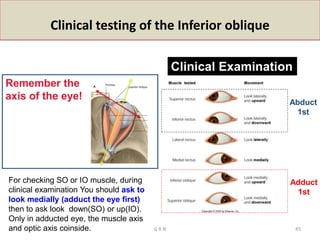
This document provides information about the extraocular muscles. It describes the seven voluntary extraocular muscles - the four rectus muscles (superior, inferior, medial, lateral), and two oblique muscles (superior, inferior). It also describes the levator palpebrae superioris muscle. For each muscle, it details their origin, course, innervation, and actions. Clinical testing techniques for each muscle are also outlined. The summary focuses on identifying the seven voluntary extraocular muscles and briefly mentioning their attachments and functions.