Downloaded 424 times
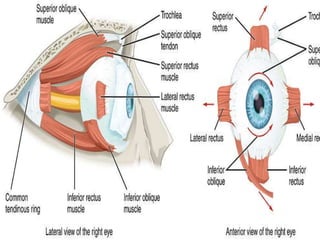
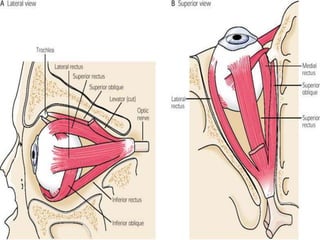
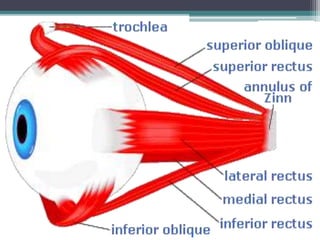
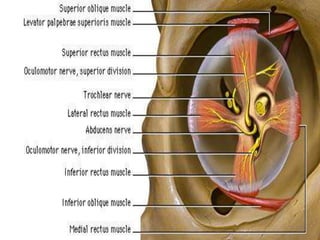
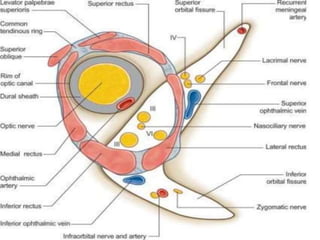
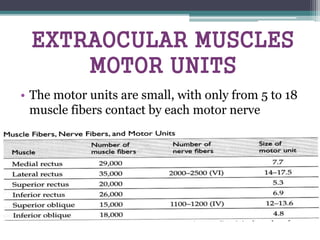
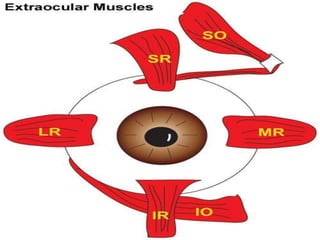
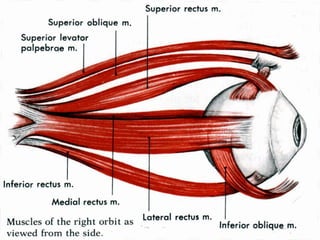
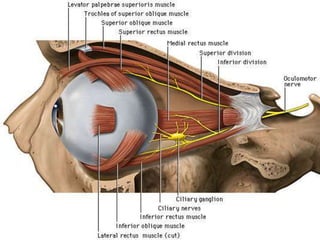
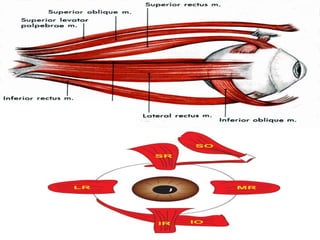
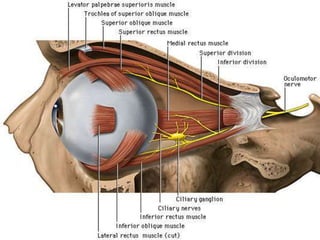
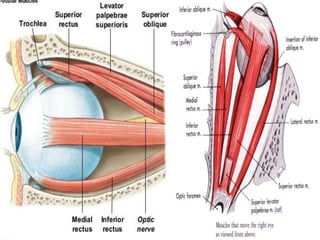
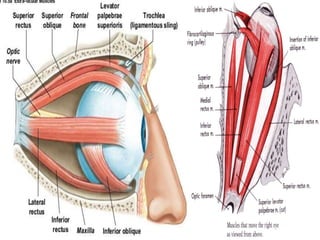
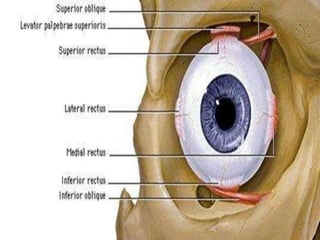
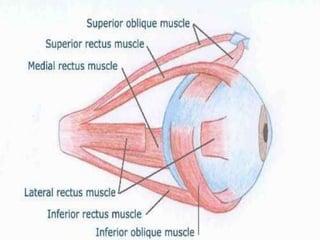
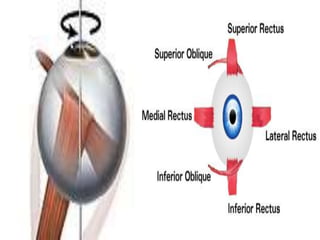
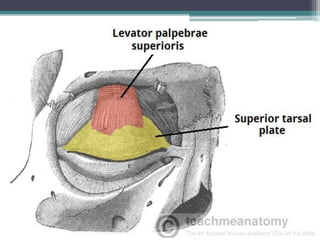
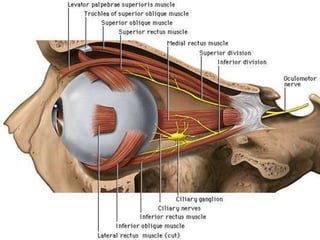
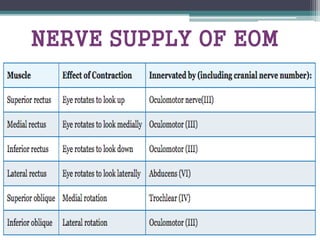
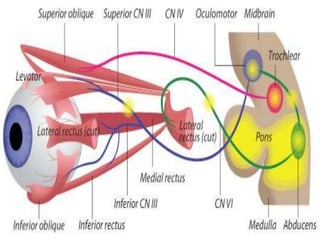
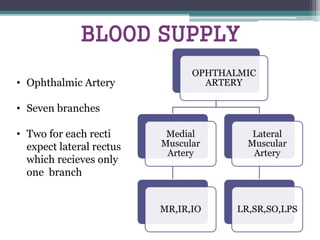
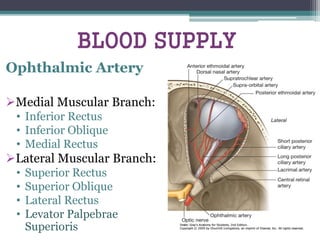

This document provides an overview of the anatomy of the extraocular muscles. It discusses the seven extraocular muscles, which can be divided into two groups: muscles responsible for eye movement (the four recti muscles and two oblique muscles) and the levator palpebrae superioris muscle responsible for eyelid elevation. For each muscle, the document outlines their origin, insertion point, blood supply, size, relationships to surrounding structures, and innervation. The recti muscles originate from the annulus of Zinn, while the oblique muscles take an angular path to the eyeball.














































































