This document provides information on exercise prescription for individuals with hypertension. It defines hypertension and its stages/grades according to different clinical guidelines. It discusses the large healthcare burden of uncontrolled hypertension. Regular physical activity and exercise are recommended as first-line interventions for both preventing and treating hypertension due to their ability to lower blood pressure through multiple physiological mechanisms. The document provides an example exercise prescription for a hypertensive population that includes aerobic and resistance training a minimum of 150 minutes per week. It also provides recommendations on exercise testing and medical supervision depending on a person's blood pressure levels and cardiovascular disease risk factors.

![Hypertension
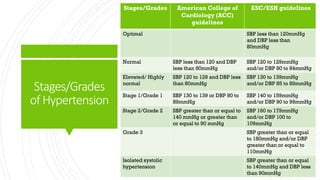
Hypertension is the most common, costly, and
preventable cardiovascular disease (CVD) risk factor.
The current definition of hypertension (HTN) is systolic
blood pressure (SBP) values of 130mmHg or more
and/or diastolic blood pressure (DBP) more than 80
mmHg. *
Prevalence of hypertension in India is at alarming level
and is estimated to account for 10.8% of all the deaths
in the country.**
*Iqbal AM, Jamal SF. Essential Hypertension. [Updated 2022 Jul 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-.
Available from: https://www.ncbi.nlm.nih.gov/books/NBK539859/
**Kurjogi MM, Vanti GL, Kaulgud RS. Prevalence of hypertension and its associated risk factors in Dharwad population: A cross-sectional study.
Indian Heart J. 2021 Nov-Dec;73(6):751-753.doi: 10.1016/j.ihj.2021.10.006.Epub 2021 Oct 22. PMID: 34695447;PMCID: PMC8642654.](https://image.slidesharecdn.com/exerciseprescriptionforhypertensivepopulation-221027065209-fb3c5892/85/Exercise-Prescription-For-Hypertensive-Population-pdf-3-320.jpg)

![AnExercise
Prescriptionfor
Hypertension
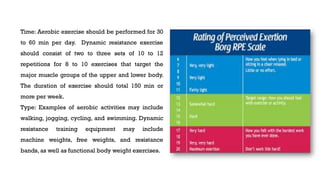
Frequency: Aerobic exercise on most, preferably all
days of the week and dynamic resistance exercise on 2
to 3 days in that same week.
Intensity: Moderate intensity aerobic exercise (i.e., 40 to
<60 % VO2max or HR reserve; 11–13 rating of
perceived exertion [RPE] on the 6–20 Borg Scale and
moderate intensity dynamic resistance exercise (60 %
to 80 % one repetition maximum [1-RM]).](https://image.slidesharecdn.com/exerciseprescriptionforhypertensivepopulation-221027065209-fb3c5892/85/Exercise-Prescription-For-Hypertensive-Population-pdf-11-320.jpg)
























































![Physiotherapy in pulmonary_surgery[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/pulmonarysurgery1-230705093621-2b78f958-thumbnail.jpg?width=640&height=640&fit=bounds)

















![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)












