Downloaded 606 times


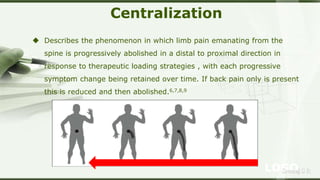


The McKenzie Method is a classification system and treatment approach developed by Robin McKenzie for back, neck, and extremity pain. It involves assessing a patient's response to various movements and positions to determine the cause of their pain and develop an individualized exercise plan. The goals are to centralize or reduce pain. There are three main syndromes - postural, dysfunction, and derangement - each with different treatments like posture correction, mobilizing exercises, or movements to induce a directional preference. The McKenzie Method aims to actively involve patients to self-manage their pain.


















![Neurophysiological facilitation of respiration [npf]](https://cdn.slidesharecdn.com/ss_thumbnails/neurophysiologicalfacilitationofrespirationnpf-180714163516-thumbnail.jpg?width=640&height=640&fit=bounds)




































































