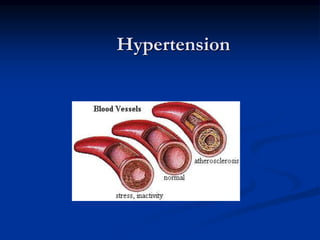
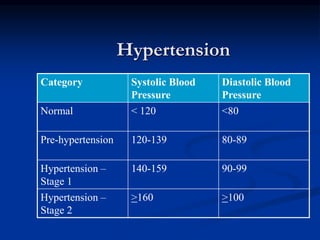
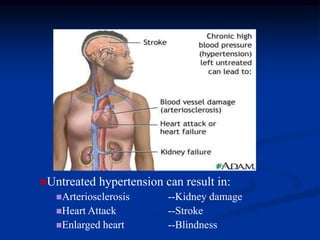
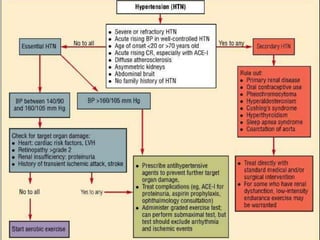
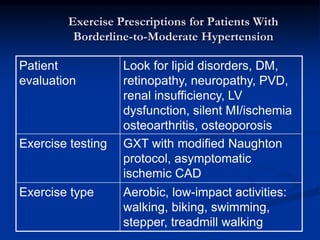
This document discusses hypertension (high blood pressure) including its causes, risk factors, diagnosis, treatment, and lifestyle modifications. It defines normal and abnormal blood pressure readings and stages of hypertension. The major factors that help regulate blood pressure are the sympathetic nervous system and kidneys. Untreated hypertension can damage organs and increase heart attack and stroke risk. Treatment involves lifestyle changes like reducing sodium and alcohol intake, exercising, and weight control as well as medications. The DASH diet is effective for lowering blood pressure. Exercise prescriptions should start gradually and avoid excessive blood pressure rises.