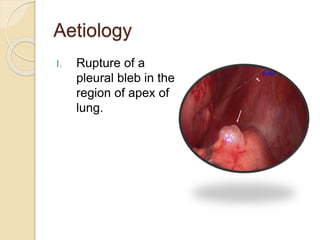
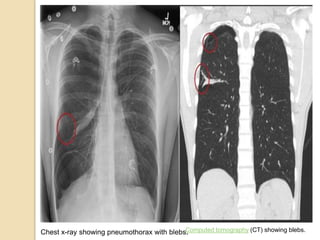
A pneumothorax occurs when air enters the pleural space between the lungs and chest wall, causing the lung to collapse. It can be caused by trauma, rupture of blebs or bullae in the lungs, or underlying lung conditions. Symptoms include chest pain and shortness of breath. On examination, findings may include diminished chest movement, absent breath sounds, and hyper-resonance on percussion. Treatment involves bed rest for small pneumothorax, needle aspiration or chest tube for large ones, and potential pleurodesis or pleurectomy for recurrent cases. Physiotherapy focuses on expansion exercises to re-expand the lung and shoulder exercises to maintain mobility.








![Physiotherapy in pulmonary_surgery[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/pulmonarysurgery1-230705093621-2b78f958-thumbnail.jpg?width=640&height=640&fit=bounds)






![Neurophysiological facilitation of respiration [npf]](https://cdn.slidesharecdn.com/ss_thumbnails/neurophysiologicalfacilitationofrespirationnpf-180714163516-thumbnail.jpg?width=640&height=640&fit=bounds)








































































