
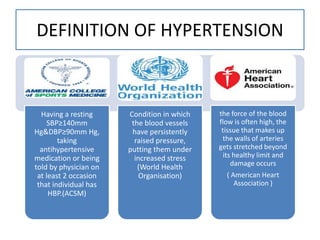







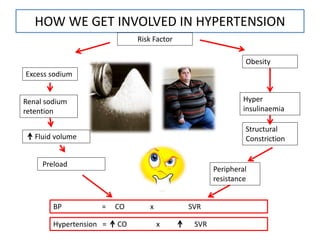

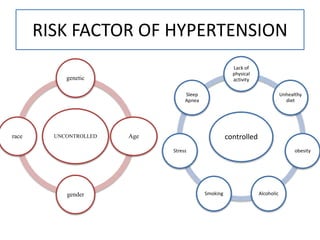









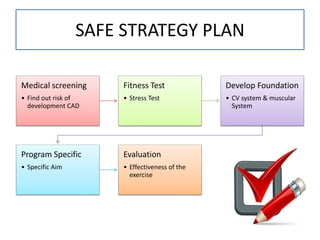
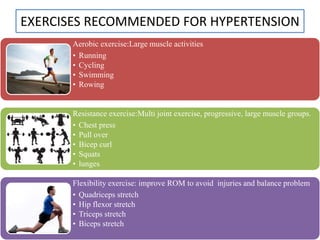



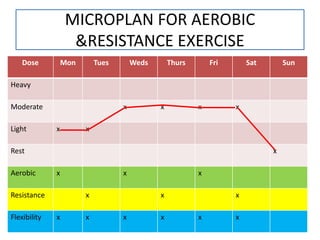
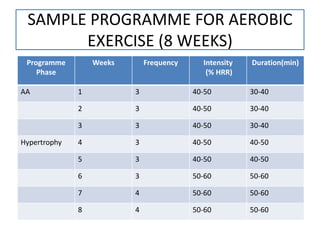










This document provides information about hypertension, including: - Definitions of hypertension from various health organizations. - Prevalence rates of hypertension globally and in Malaysia, which is higher in urban vs. rural areas. - Risk factors, symptoms, complications and classifications of hypertension. - Recommended tests for diagnosing hypertension including ambulatory blood pressure monitoring and stress tests. - Lifestyle modifications to manage hypertension including the DASH diet, physical activity, and aerobic and resistance exercise programs. The goal is to lower blood pressure through a combination of diet, exercise and medications in order to reduce risks of complications like heart attack and stroke. Regular physical activity and following the DASH diet are important























































































