This document summarizes several types of supraventricular arrhythmias (abnormalities of impulse generation or conduction above the ventricles), including:
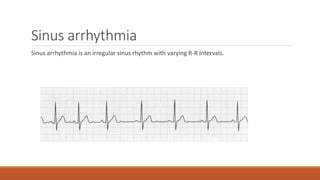
- Sinus arrhythmia, where the heart rate varies due to breathing
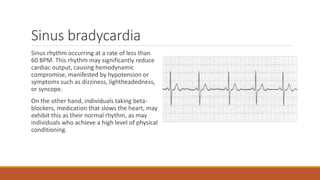
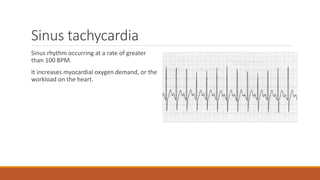
- Sinus bradycardia, a slow heart rate below 60 BPM, and sinus tachycardia, a fast heart rate over 100 BPM
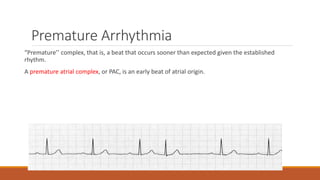
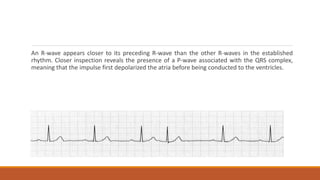
- Premature beats that occur earlier than expected, such as premature atrial complexes or premature junctional complexes
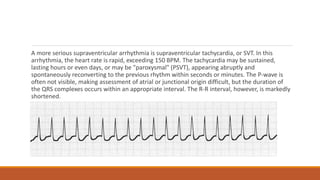
- Supraventricular tachycardia, a rapid heart rate over 150 BPM that can be sustained or paroxysmal
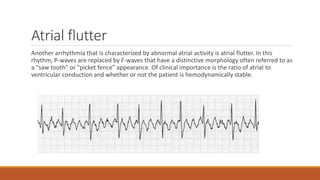
- Atrial flutter, where the normal P-waves are replaced by



































![Shadechapter09.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter09-150421103043-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)






















![Physiotherapy in pulmonary_surgery[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/pulmonarysurgery1-230705093621-2b78f958-thumbnail.jpg?width=640&height=640&fit=bounds)





























