Download as PDF, PPTX
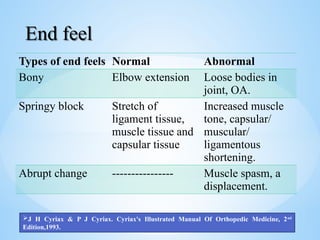
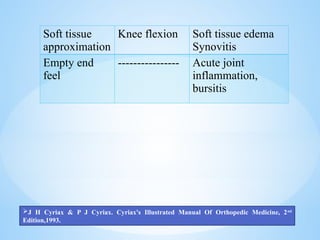
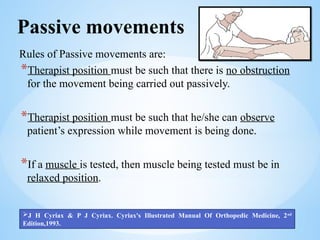
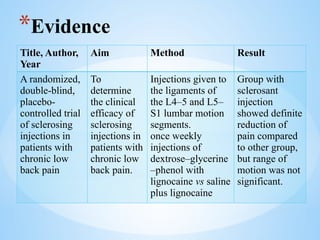
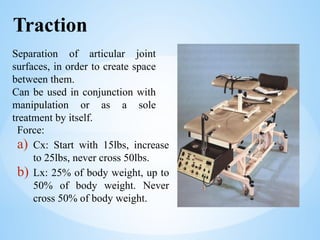
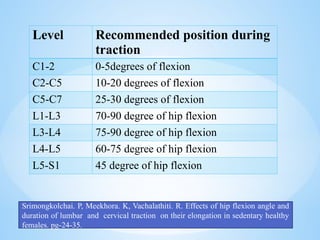
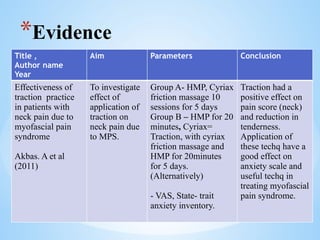
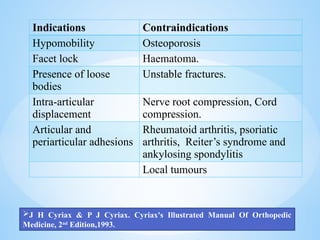

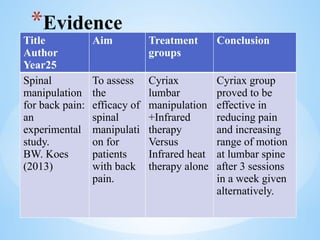
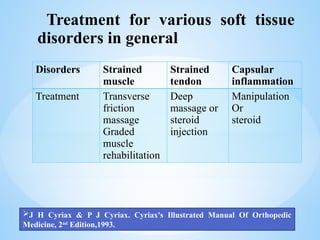
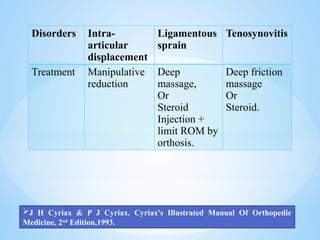

The document discusses the Cyriax method, a manual therapy approach developed by James Cyriax in the 1890s, which focuses on diagnosing and treating musculoskeletal disorders through selective tissue tension and various therapeutic techniques. Key principles include understanding the roles of inert and contractile soft tissue structures, applying specific treatments like transverse friction massage, traction, and manipulation, and assessing pain types and responses to guide therapy. It also covers the indications, contraindications, and evidence regarding the efficacy of these treatments for various conditions.























































































