Downloaded 81 times






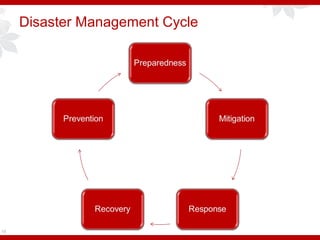
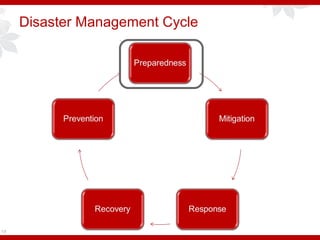



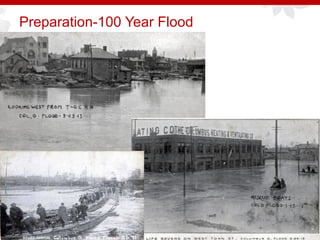

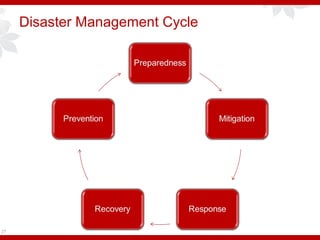
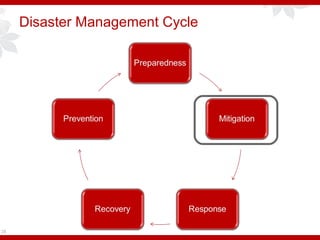

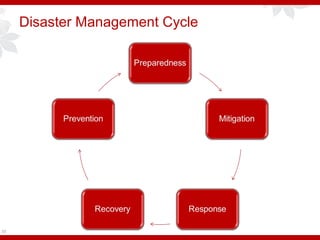
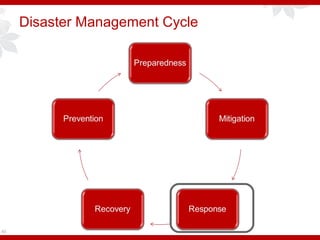


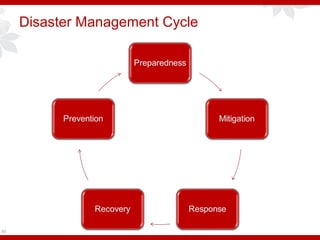
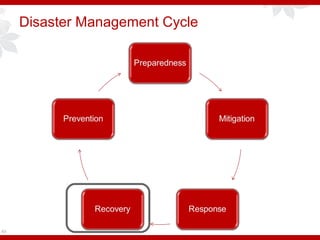

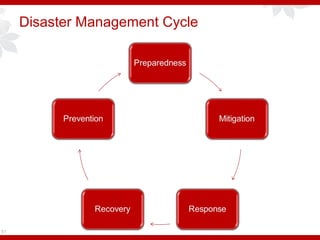
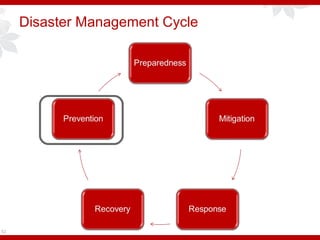


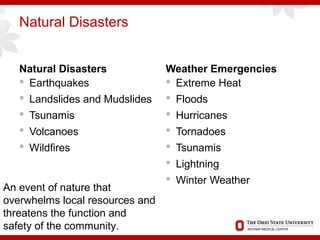


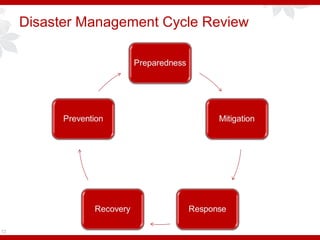
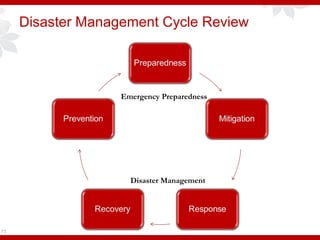


This document provides an overview of emergency response to natural disasters since 9/11. It discusses key aspects of the disaster management cycle including preparation, mitigation, response, recovery and prevention. Specific natural disasters like floods, winds and earthquakes are examined. Injury patterns from collapsed buildings, winds and flooding are defined. The importance of preparation, having an incident command system and surge capacity plan are emphasized.

































































































