The document outlines several key principles and phases of disaster management:
- Principles include that disaster management is a shared responsibility across all levels of government, uses existing day-to-day resources, involves organizations playing roles aligned with their core functions, and recognizes the roles of individuals and non-government agencies.
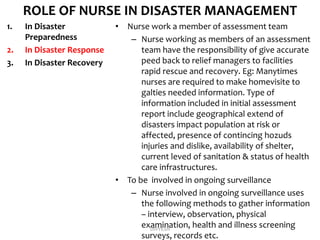
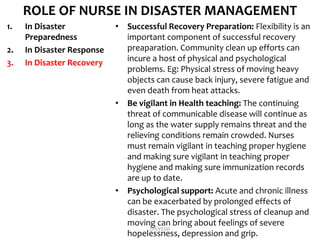
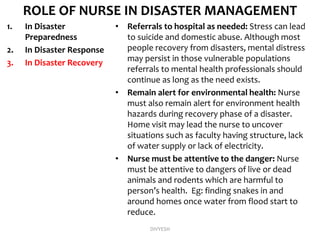
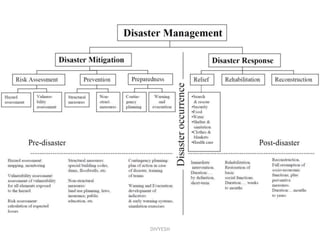
- Phases include preparedness, impact assessment, response (including relief and rehabilitation), and mitigation. Response involves search and rescue, field care, triage (including sorting casualties into immediate, delayed, minor, and expectant categories based on need), and medical treatment. International and non-profit agencies also play roles.





















![Disaster management[1]](https://cdn.slidesharecdn.com/ss_thumbnails/disastermanagement1-170312140415-thumbnail.jpg?width=640&height=640&fit=bounds)































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)















