Downloaded 15 times
![Epidemiology [Distribution]
• TIME:
• More common in rainy season.
• PLACE:
• Poor sanitation.
• Flies.
• Contaminated water and food.
• Poor housing.
• Overcrowding during marriages and fairs.](https://image.slidesharecdn.com/cholera-200608123341/85/Epidemiology-and-Control-Measures-for-Cholera-8-320.jpg)
![Epidemiology [Distribution]
• PERSON:
• Age:
• Cholera affects all ages.
• Gender:
• Affects both sexes.
• Gastric acidity:
• It is as effective barrier. Conditions that reduces acidity cause increased
susceptibility to cholera.
• Blood types:
• O>> B > A > AB](https://image.slidesharecdn.com/cholera-200608123341/85/Epidemiology-and-Control-Measures-for-Cholera-9-320.jpg)
![EPIDEMIOLOGY [DISTRIBUTION]
• PERSON:
• Economic Status:
• Low socio-economic persons are more prone.
• Education:
• Lack of education increases the risk.
• Personal Hygiene:
• Poor hygiene also increases the risk.](https://image.slidesharecdn.com/cholera-200608123341/85/Epidemiology-and-Control-Measures-for-Cholera-10-320.jpg)
![EPIDEMIOLOGY [DETERMINANTS]
• PRIMARY DETERMINANTS:
• Agent:
• The etiological agent is Vibrio Cholera and has 2 major biotypes: classical and El Tor,
Currently, El Tor is the predominant cholera pathogen worldwide.
• Has over 150 identified serotypes based on O-antigen
• Only O1 and O139 are toxigenic and cause Cholera disease (Water-borne illness)
• Resistance:
• Boiling for few seconds kills Vibrio Cholera.
• Toxin Production:
• Vibrio Cholera multiplies in the small intestine of human and produces an exotoxin (
enterotoxin ) that produces diarrhea.](https://image.slidesharecdn.com/cholera-200608123341/85/Epidemiology-and-Control-Measures-for-Cholera-11-320.jpg)
![Epidemiology [Determinants]
• SECONDARY DETERMINANTS:
• Poor hygiene and sanitation.
• Large Families and Flies.](https://image.slidesharecdn.com/cholera-200608123341/85/Epidemiology-and-Control-Measures-for-Cholera-12-320.jpg)



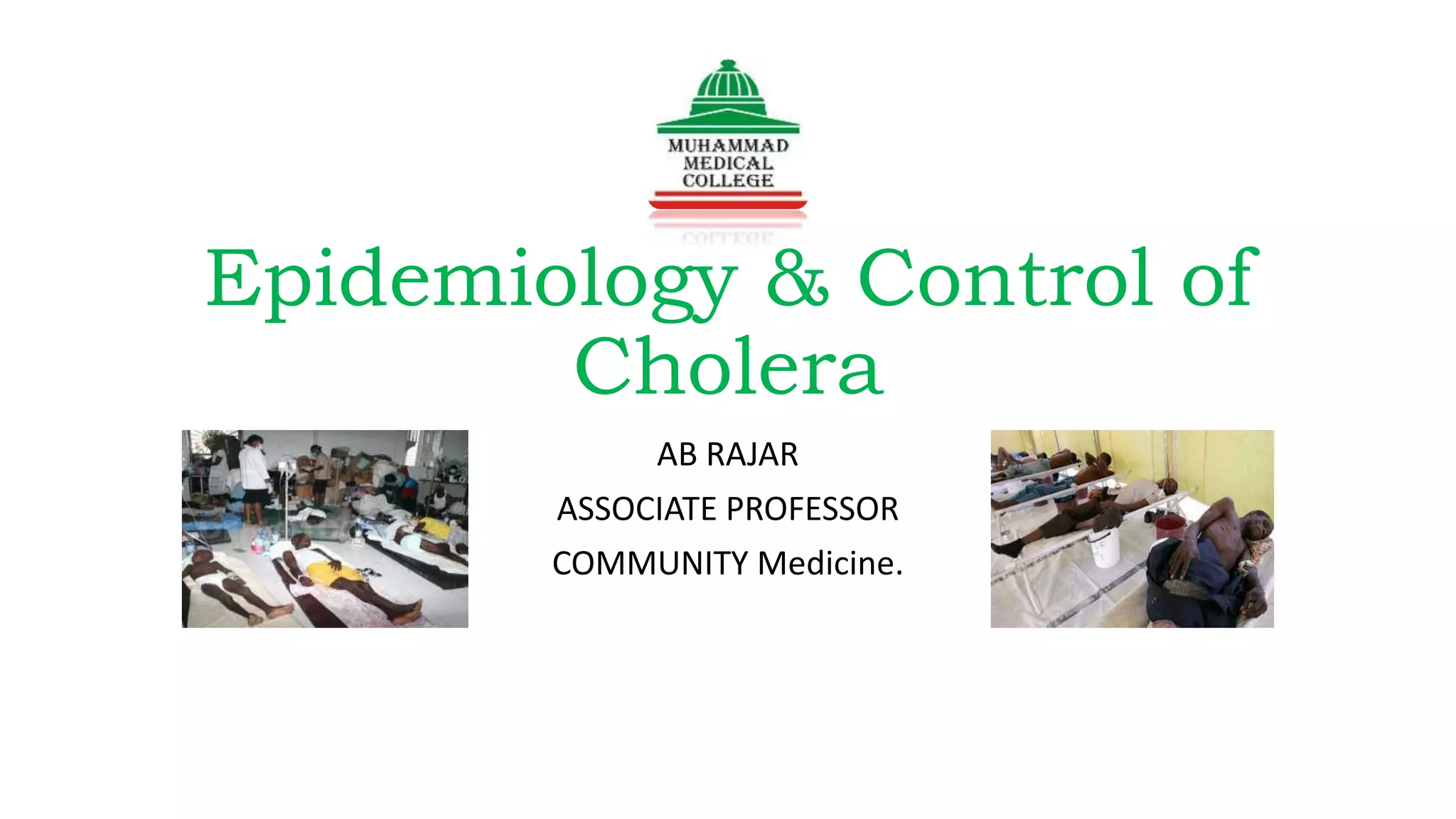
Cholera, caused by the bacterium Vibrio cholerae, primarily spreads through contaminated water and food, leading to severe watery diarrhea and vomiting. Globally, it affects 3-5 million people yearly, resulting in approximately 100,000-130,000 deaths, predominantly in the developing world. Control measures include proper sanitation, early case identification, and treatment with rehydration therapy and antibiotics.























































































