![These questions can be referred to as:
Case definition [what]
Person [who]
Place [where]
Time [when]
Causes [why]
PROFESSOR DR AB RAJAR 38](https://image.slidesharecdn.com/basicprinciplesofepidemiology-230313040910-236913f3/85/BASIC-PRINCIPLES-OF-EPIDEMIOLOGY-pptx-38-320.jpg)


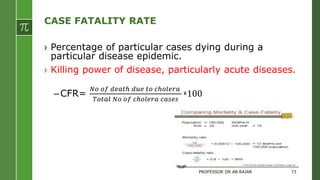
![RATIO.
› In a class that has 20 male students and 80 female
students.
› We can think about this in several ways.
› The ratio of boys to girls as 20:80 or 20/80.
› Aa 1:4 ratio (or 1/4 ratio). [This indicates that for every
boys, there are four girls].
› From the inverse perspective, i.e., the number of girls
relative to the number of boys; in this case the ratio of girls
to boys is 80/20 which is equivalent to 4 to 1, i.e., there are
four girls for every boys.
PROFESSOR DR AB RAJAR 81](https://image.slidesharecdn.com/basicprinciplesofepidemiology-230313040910-236913f3/85/BASIC-PRINCIPLES-OF-EPIDEMIOLOGY-pptx-81-320.jpg)

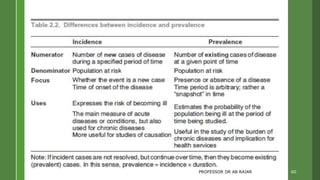
This document outlines key learning objectives for fourth-year MBBS students on the subject of epidemiology, including its definitions, aims, and essential concepts. It emphasizes the importance of epidemiology in understanding disease distribution, determining health-related states, and applying this knowledge to public health practices. Additionally, the document discusses basic measurements in epidemiology, such as incidence and prevalence, and their role in health status evaluation and disease prevention.













































![Introduction to Epidemiology.pptx [Repaired].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/1-230126203730-23334872-thumbnail.jpg?width=640&height=640&fit=bounds)









































