Download to read offline

![CASE-CONTROL STUDY [Retrospective Studies]
• A case-control study is an observational study in which
subjects are sampled based on the presence or absence of
disease and then their prior exposure status is determined.
• A case-control study involves two populations – cases and
controls and has three distinct features:
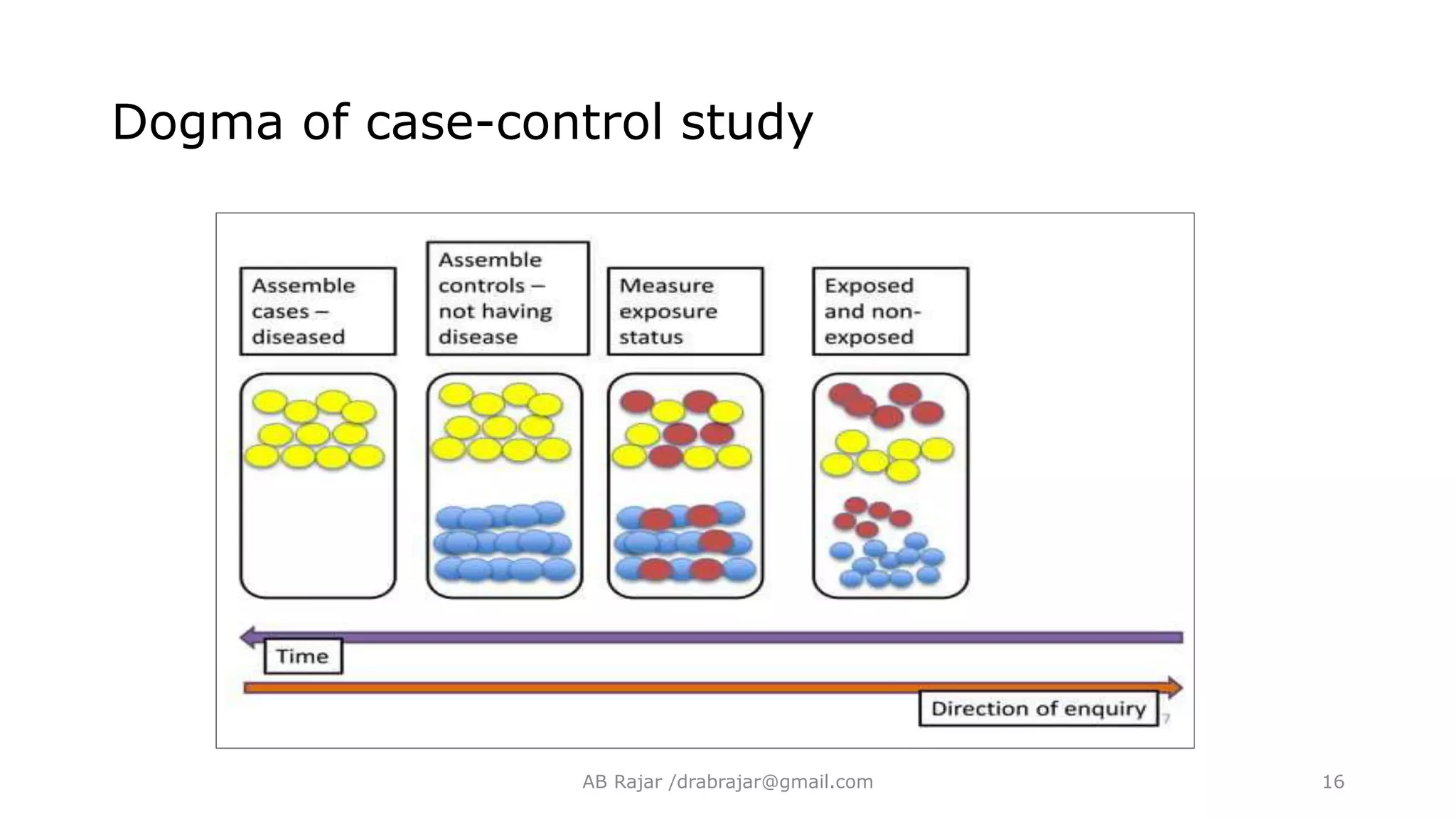
I. Both exposure and outcome occurred before the start of the
study.
II. The study proceeds backward from effect to cause.
III.It uses a control or comparison group to support or refute
an inference.
AB Rajar /drabrajar@gmail.com 14](https://image.slidesharecdn.com/case-controlstudydesign-230313093306-d5bff7ed/75/Case-Control-Study-Design-pptx-14-2048.jpg)





![Bias in Case-Control Study
• Recall Bias: [usually in case control studies].
• Cases who are aware of their disease status may be
more likely to recall exposure than controls.
• E.g, congenital malformation with prenatal infections
• Results in misclassification.
AB Rajar /drabrajar@gmail.com 59](https://image.slidesharecdn.com/case-controlstudydesign-230313093306-d5bff7ed/75/Case-Control-Study-Design-pptx-59-2048.jpg)


The document outlines a comprehensive overview of case-control studies, detailing their definition, design, and historical examples that validate their significance in epidemiological research. It discusses the selection of cases and controls, the importance of matching variables, and methods to measure exposure and analyze results, including odds ratios and biases. Key historical cases such as thalidomide and lung cancer are used to illustrate the application and effectiveness of case-control studies in confirming hypotheses about health-related risks.
Introduction by Professor Dr. AB Rajar, outlining essential learning objectives for the presentation.
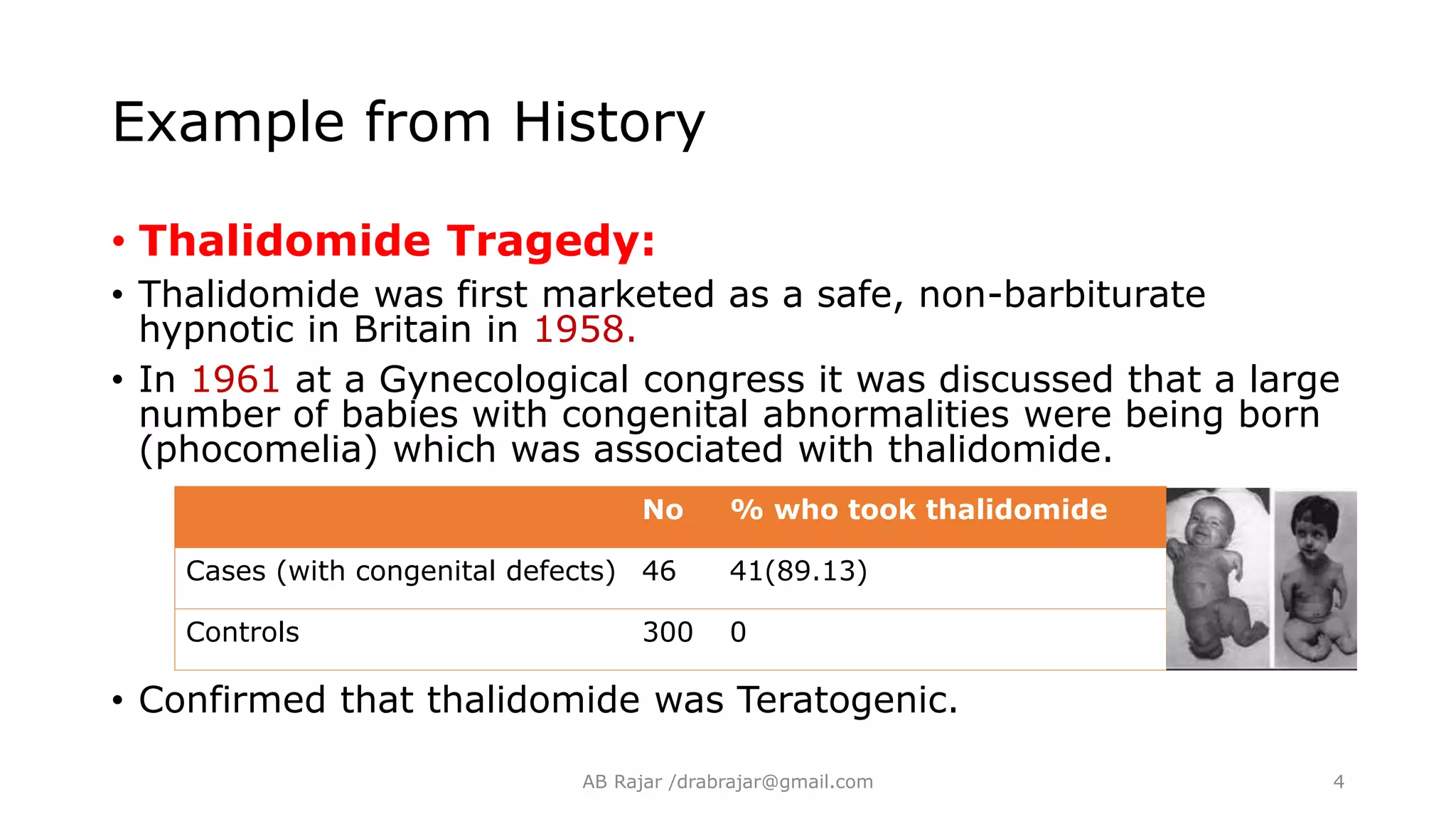
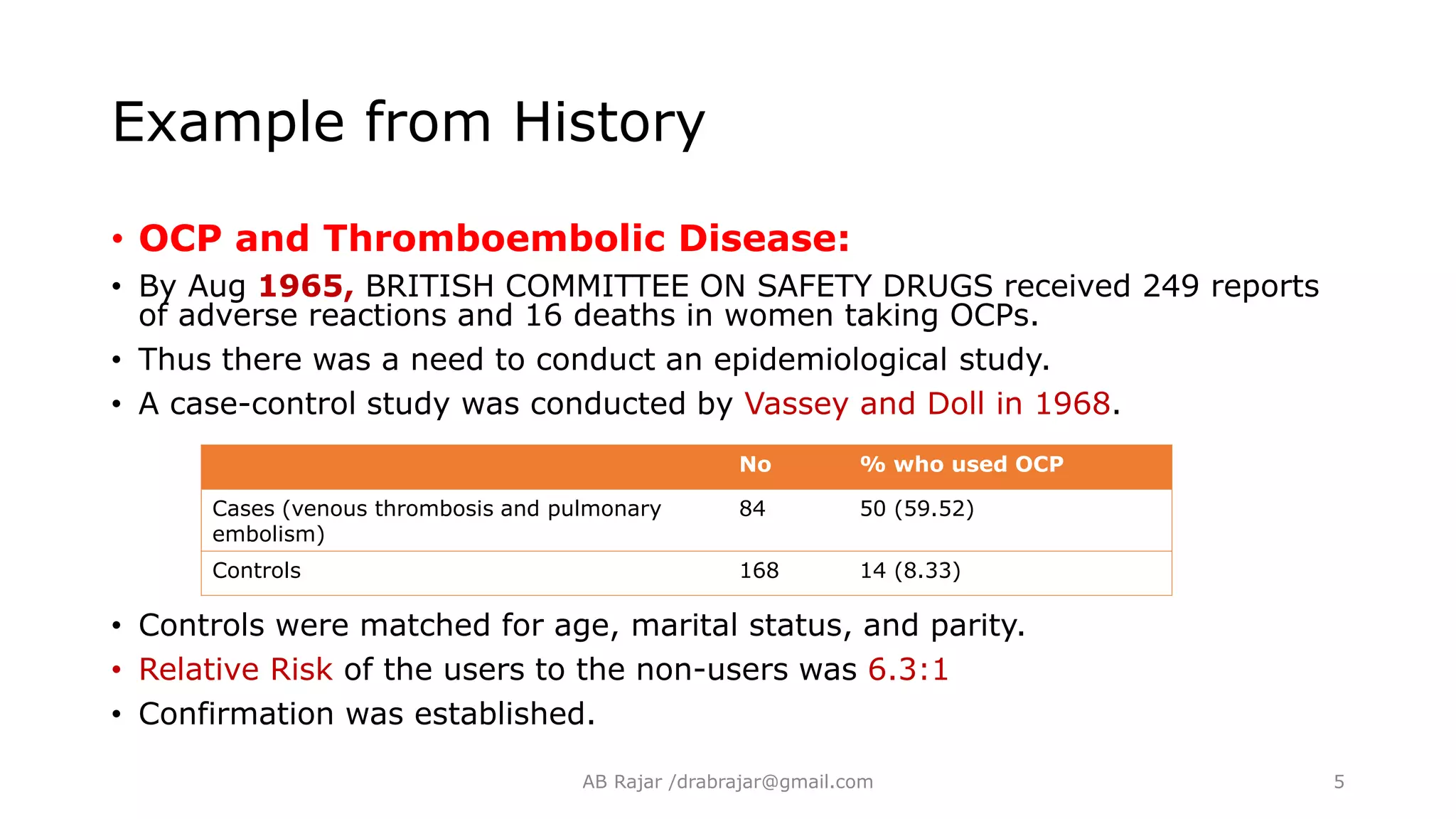
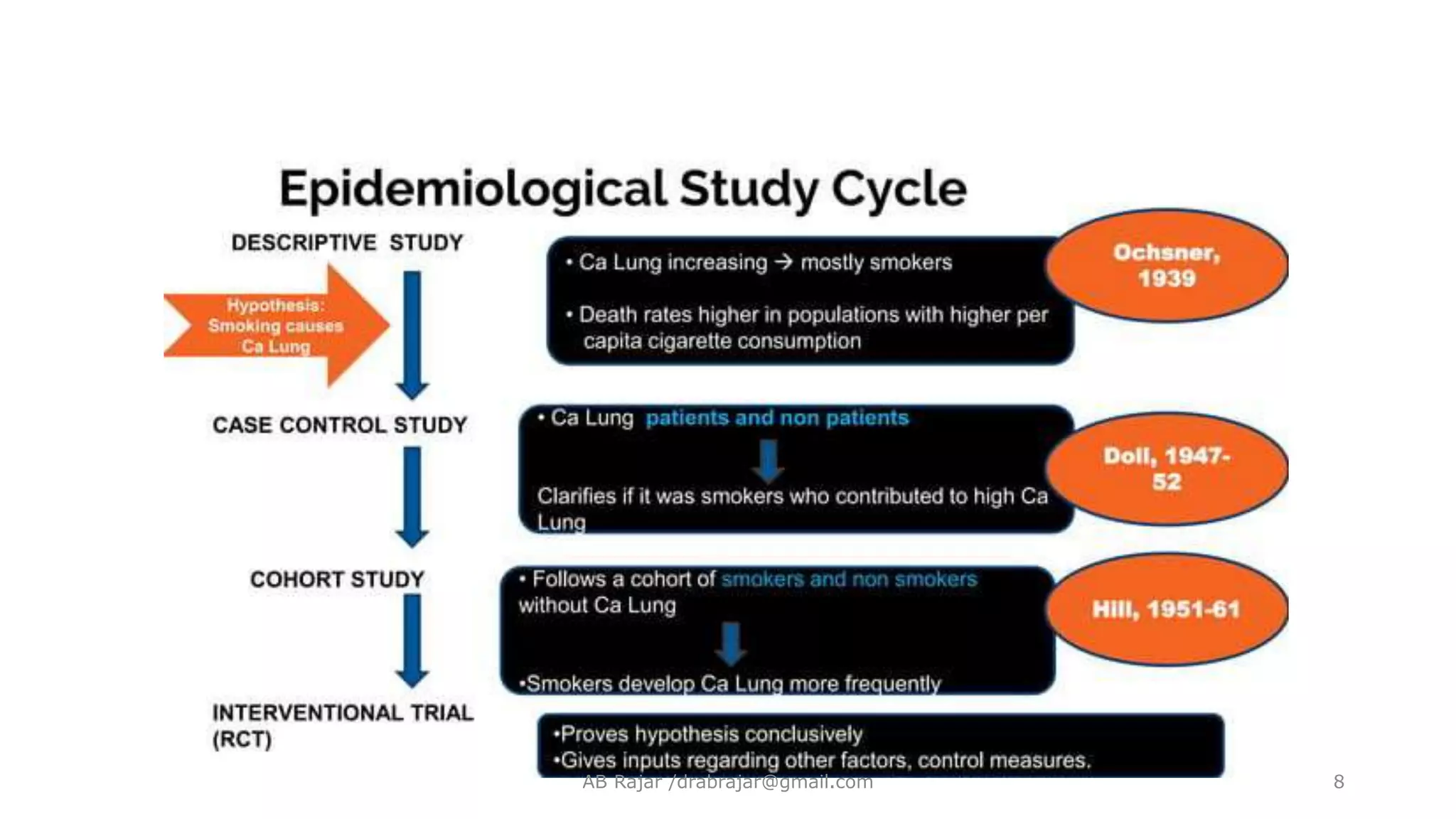
Historical context using real cases (Thalidomide, OCP, Gregg's observation) to demonstrate how hypotheses about disease exposure evolve.
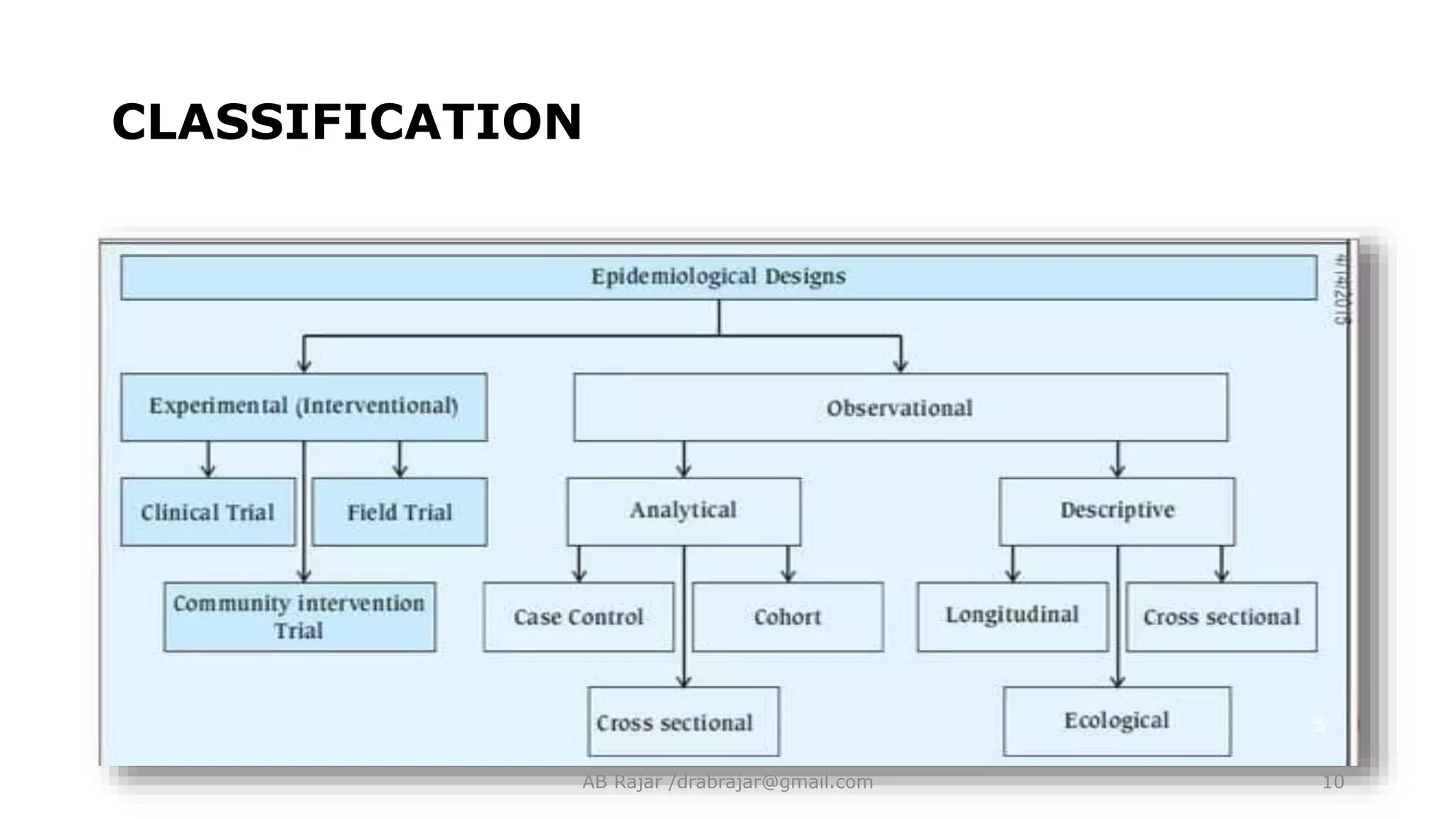
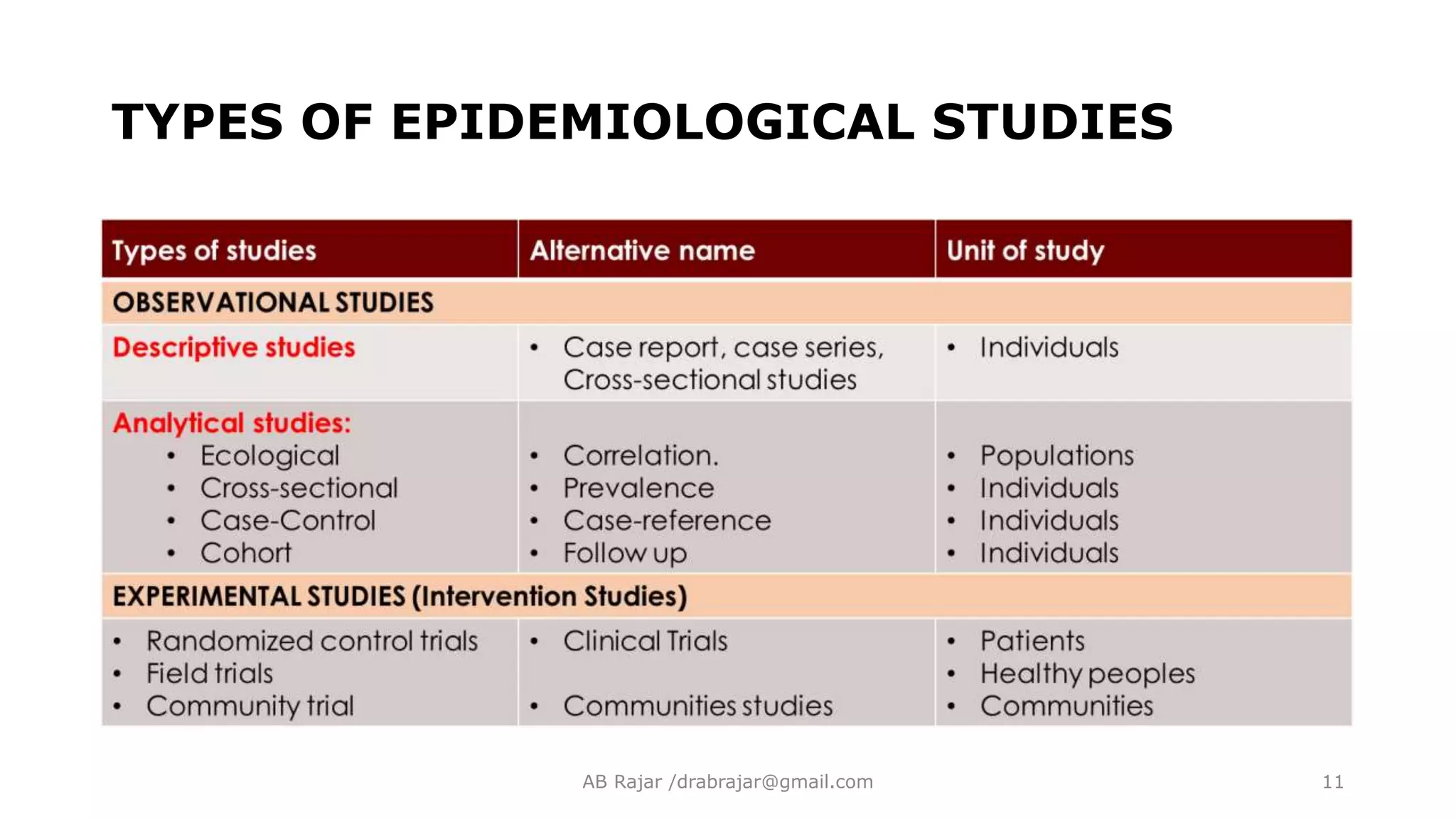
Defining epidemiology and its classification, emphasizing the need to understand health-related distributions and determinants.
Discussion on analytical studies focusing on hypothesis testing and case-control study methodology to evaluate disease exposure associations.
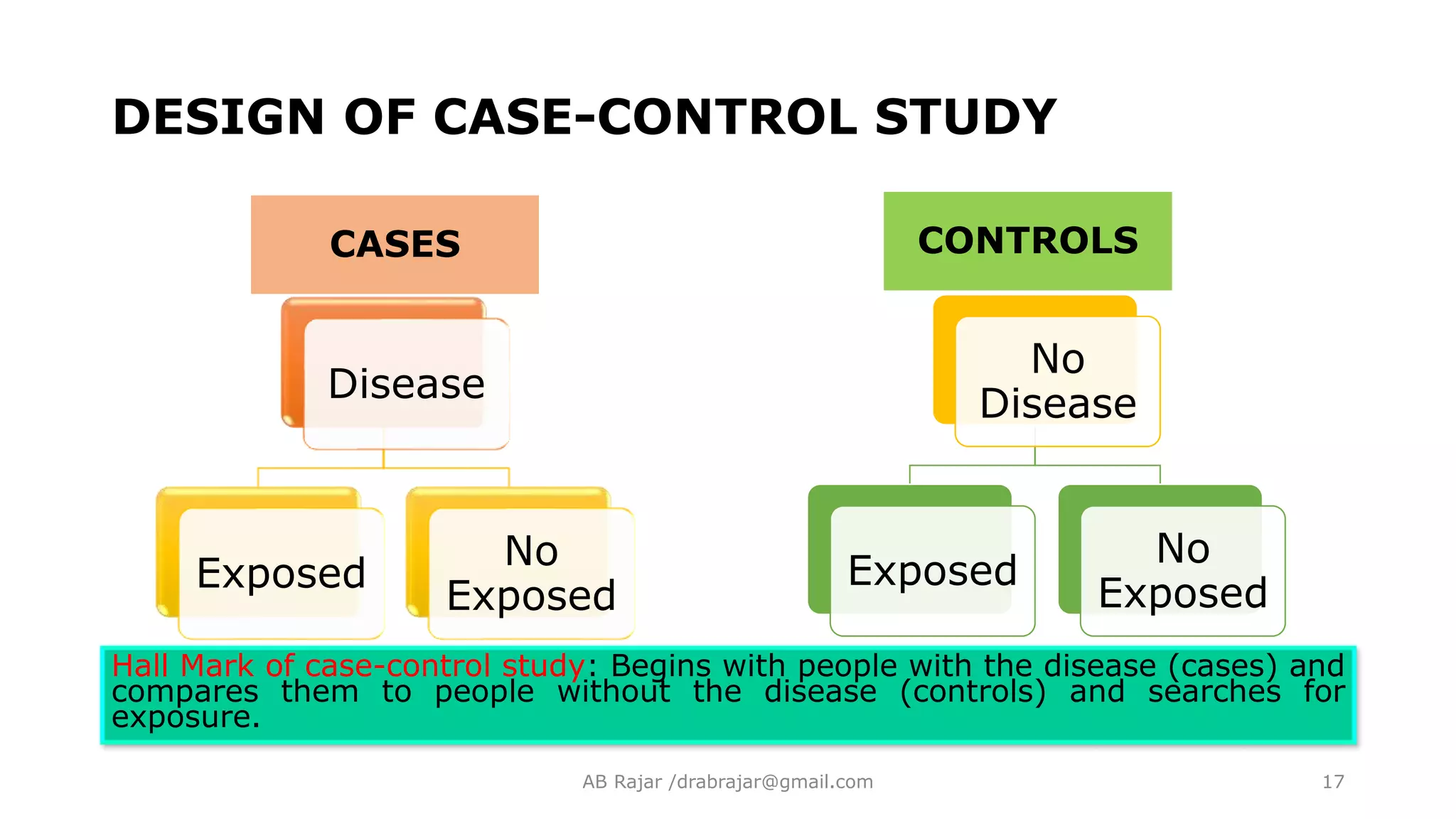
Describes the design and selection process of case-control studies, highlighting the importance of comparing cases to controls.
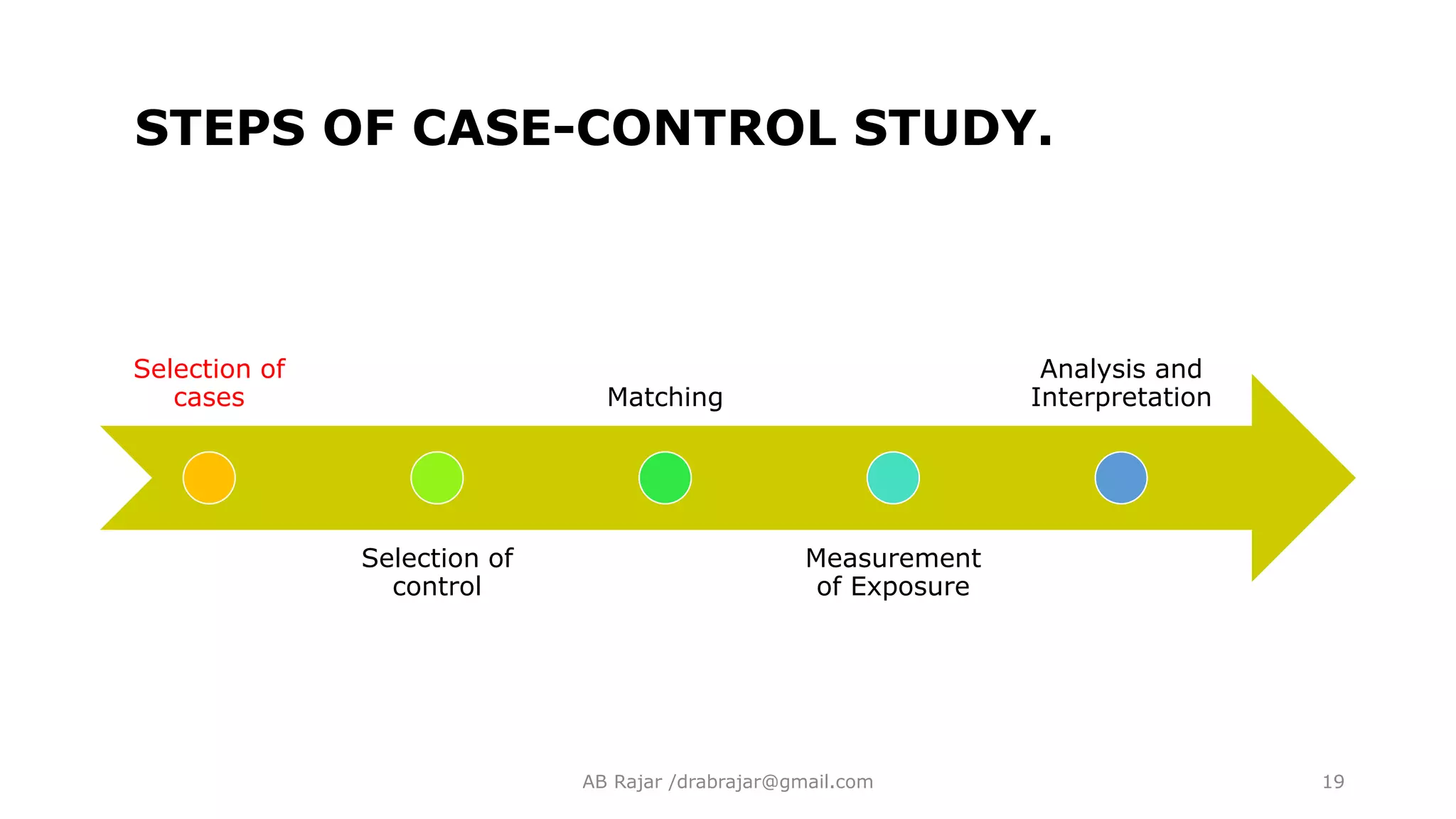
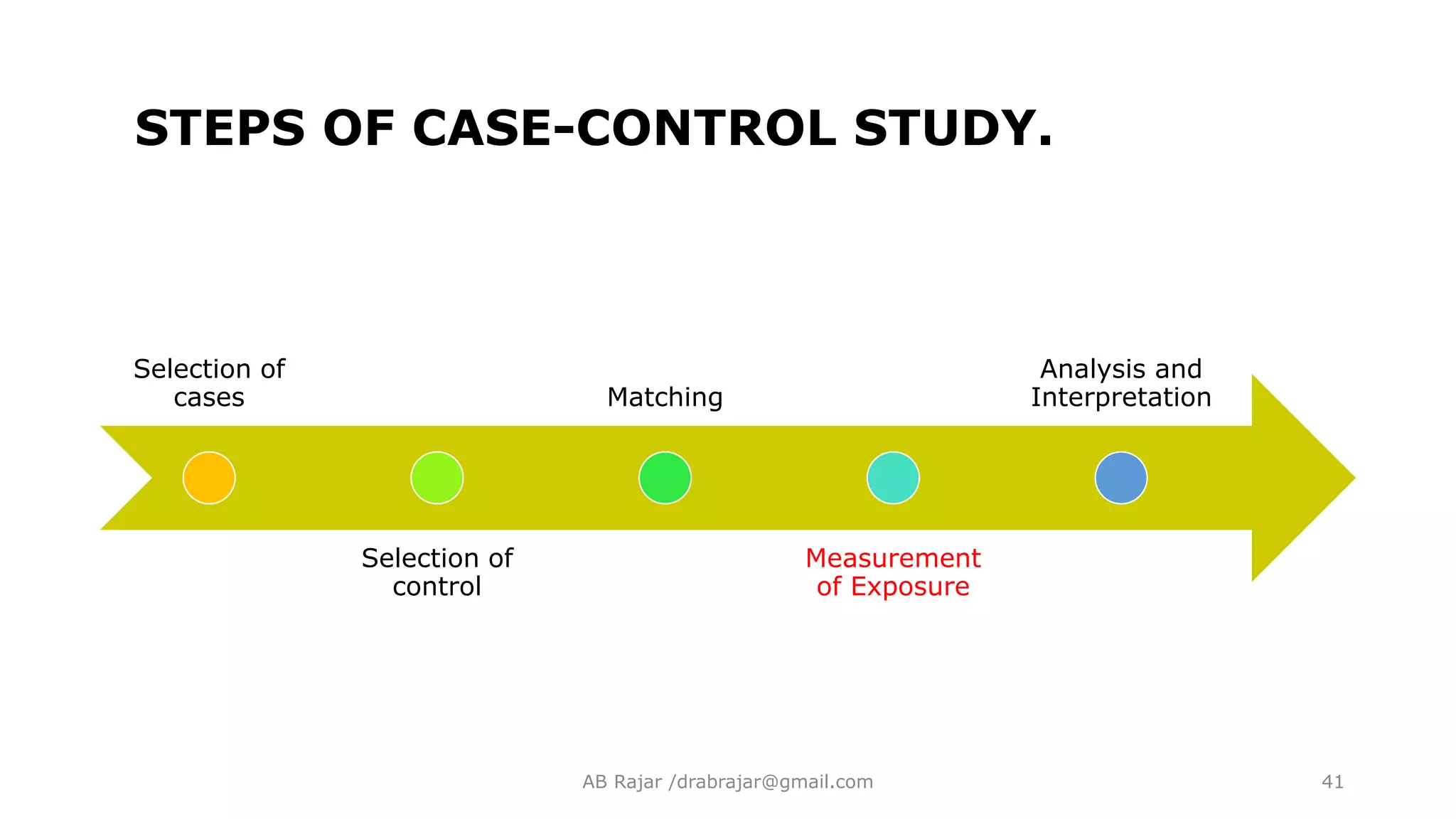
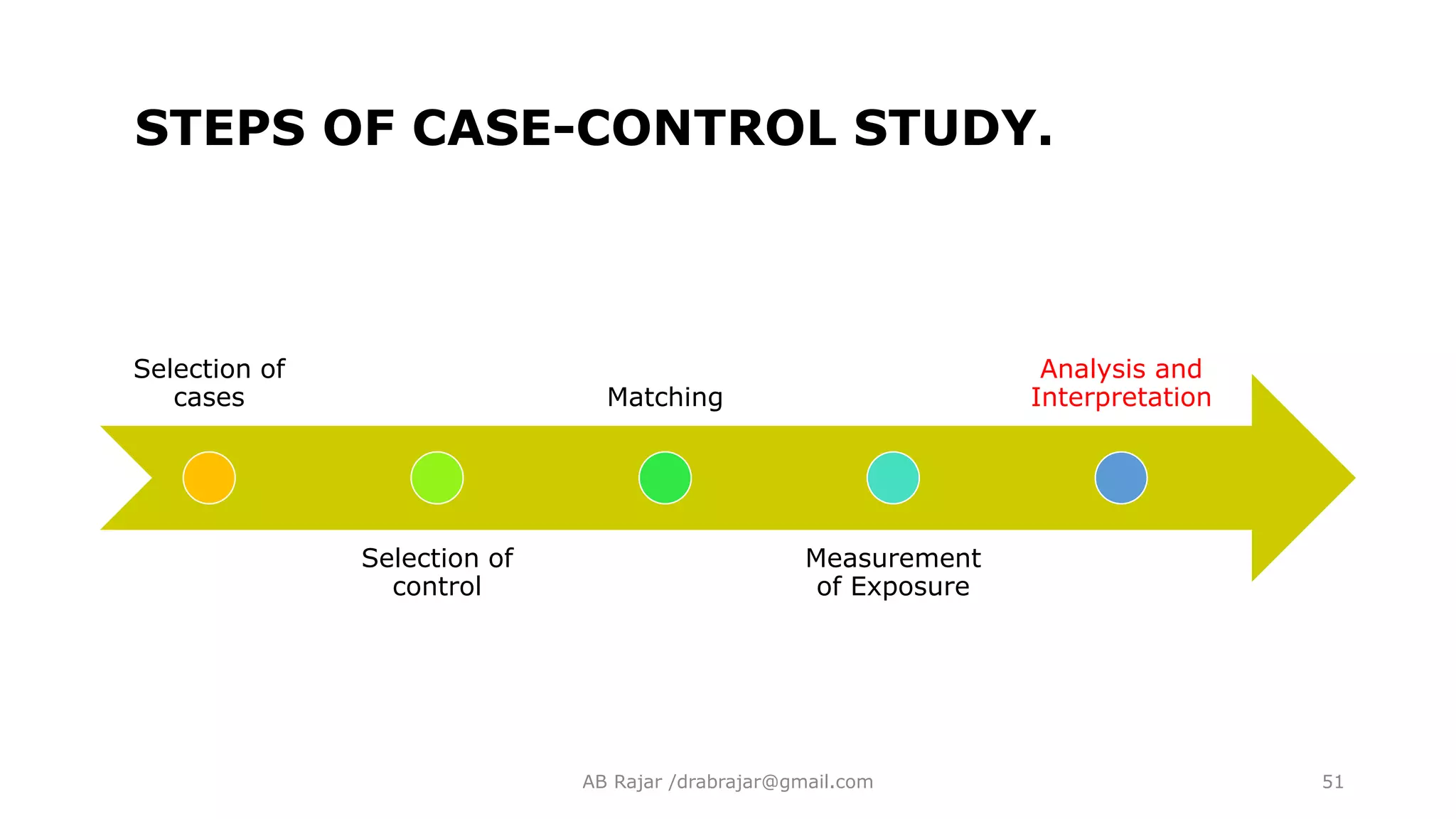
Outlines key steps, including the selection of cases and controls, accuracy in diagnostic and eligibility criteria.
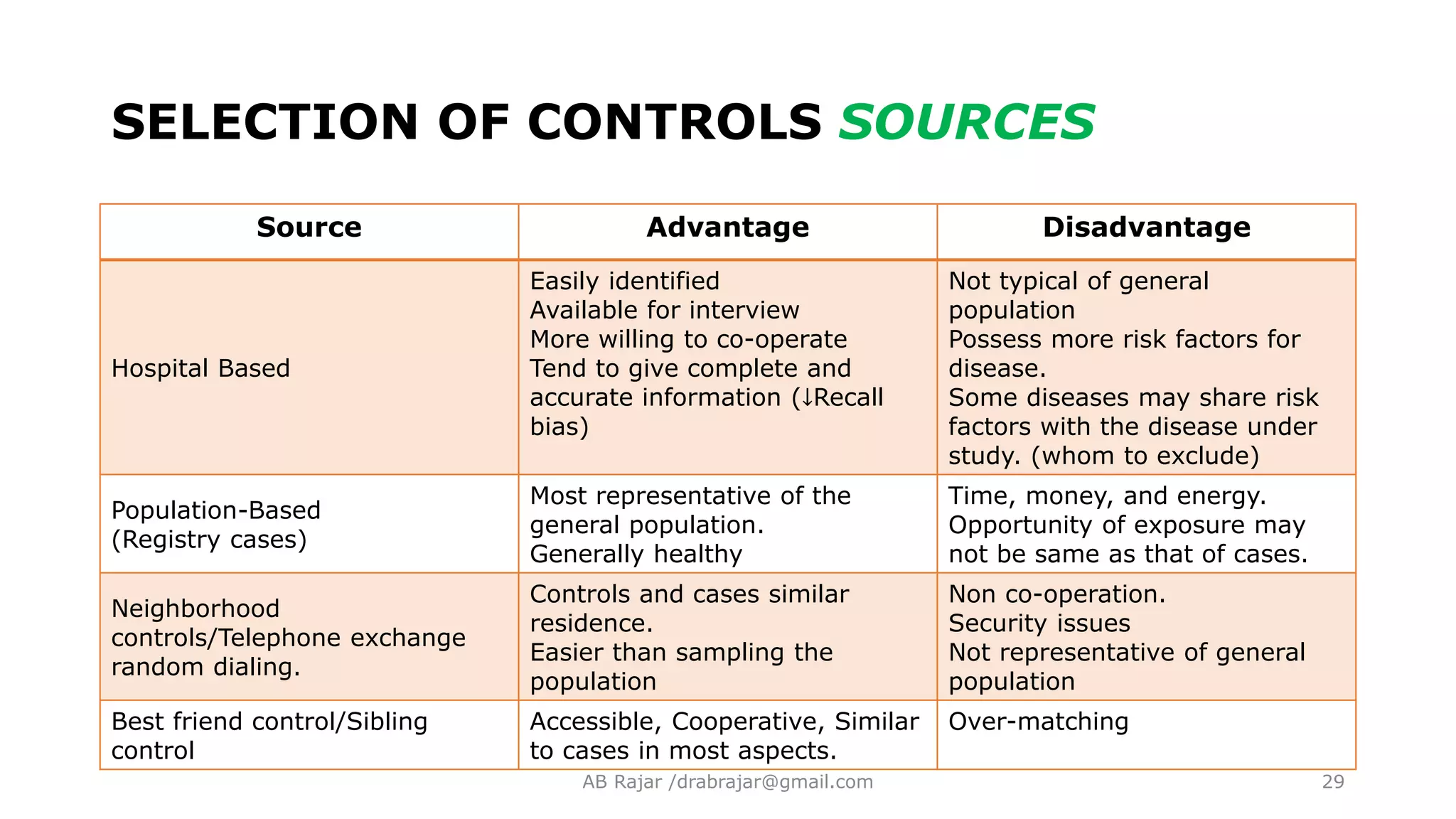
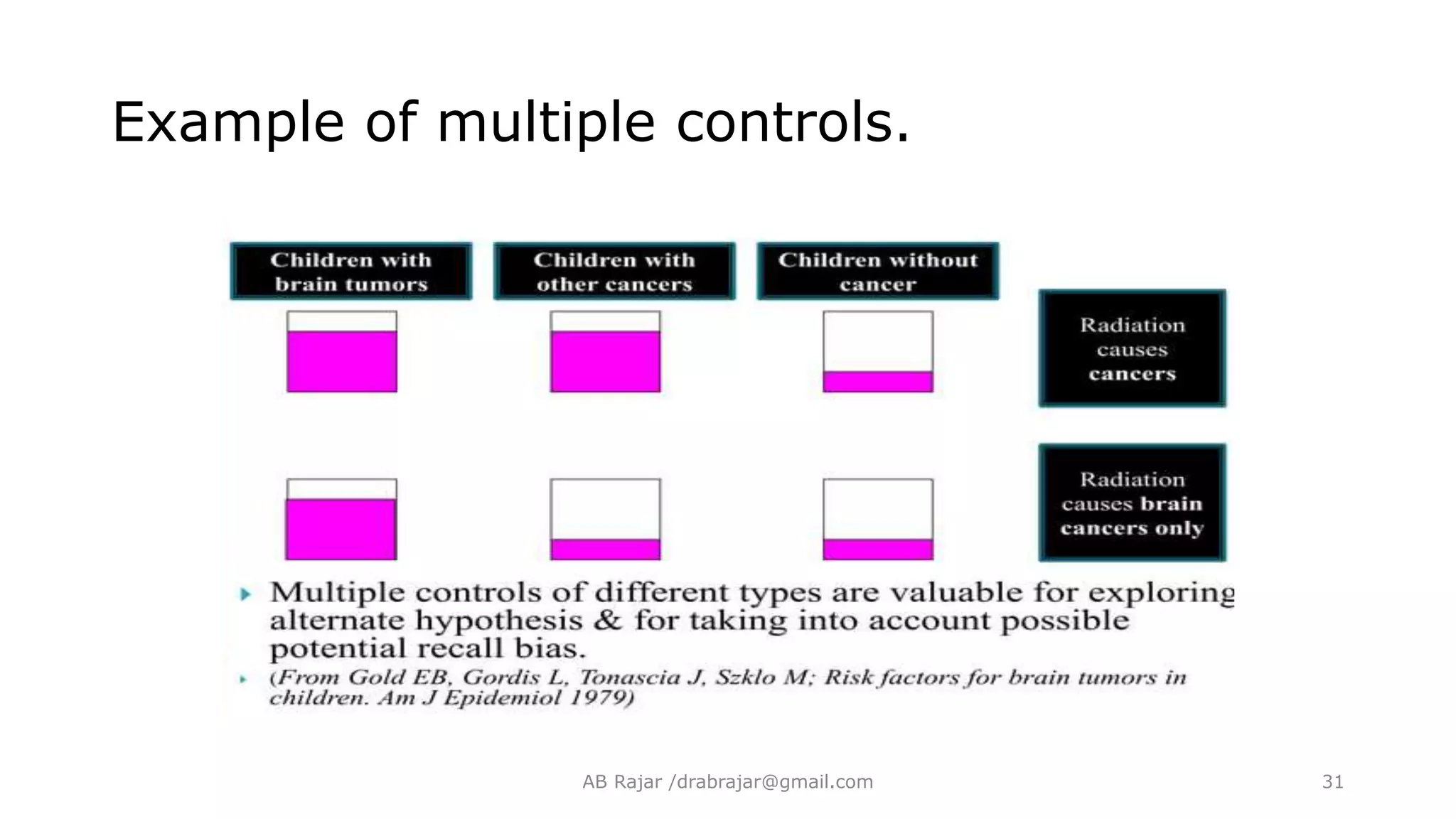
Discusses various sources of controls, their characteristics, and the importance of maintaining comparability and representativeness.
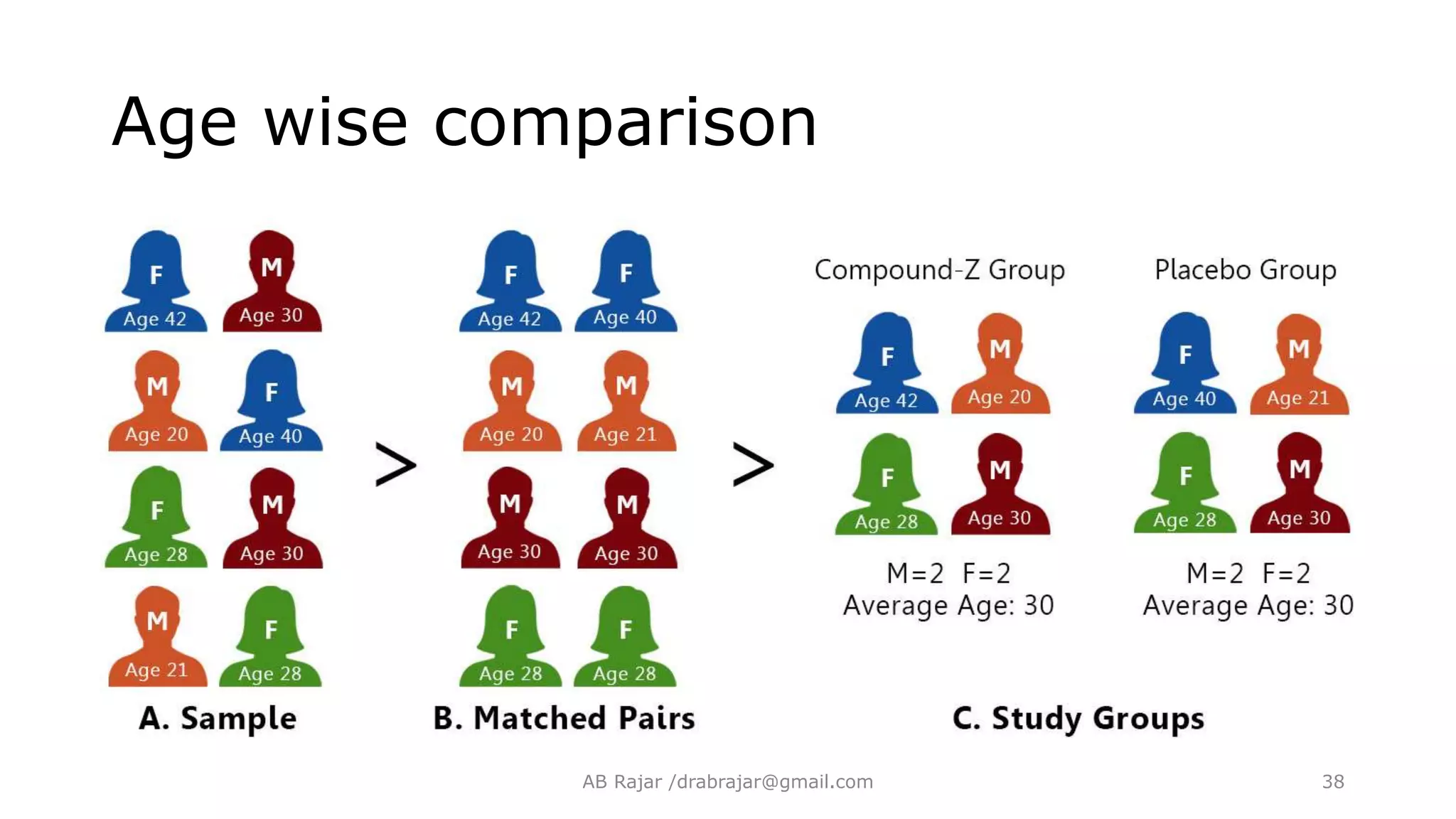
Describing the process of matching to control for variables that may affect study outcomes, distinguishing between individual and group matching.
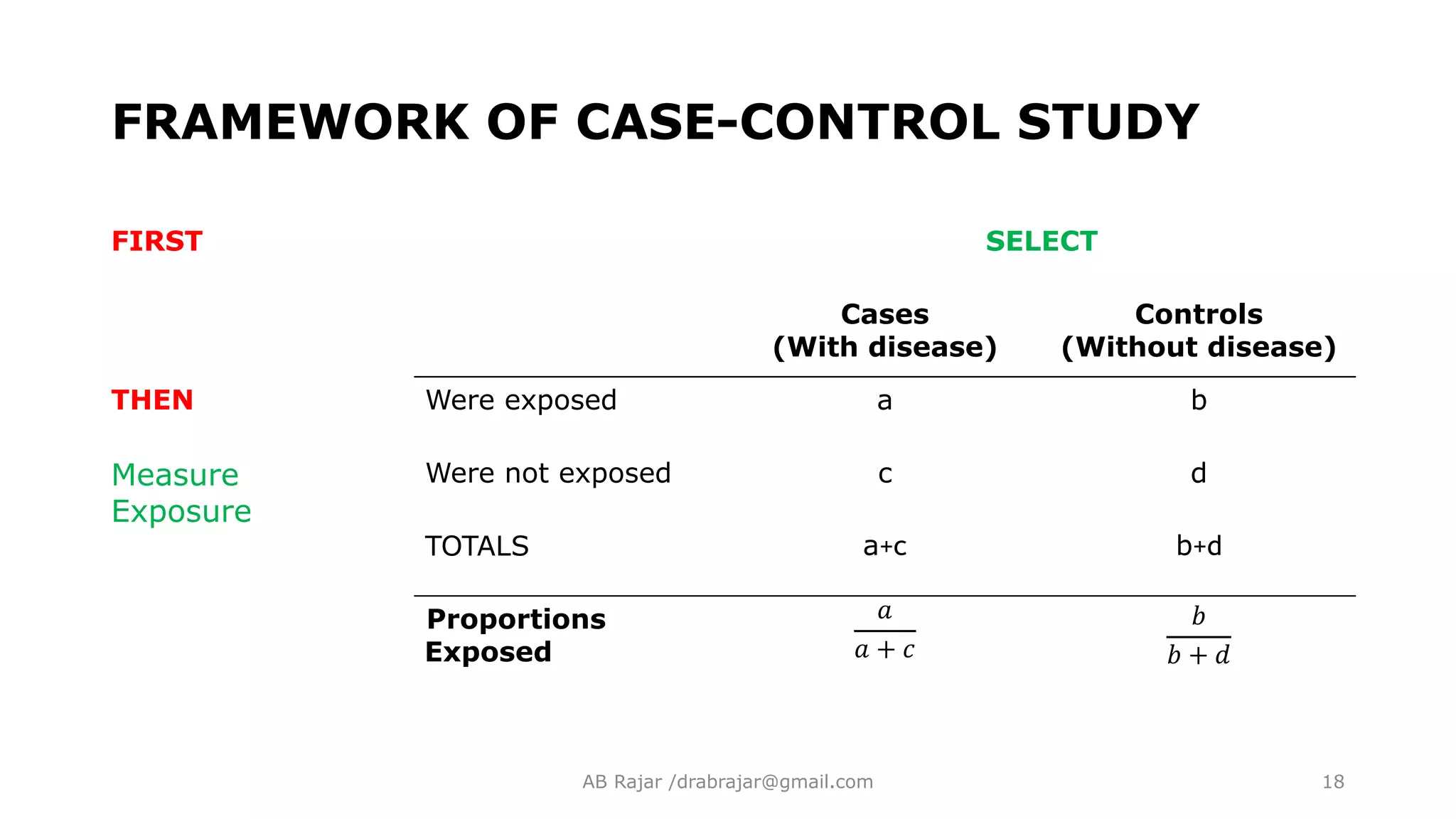
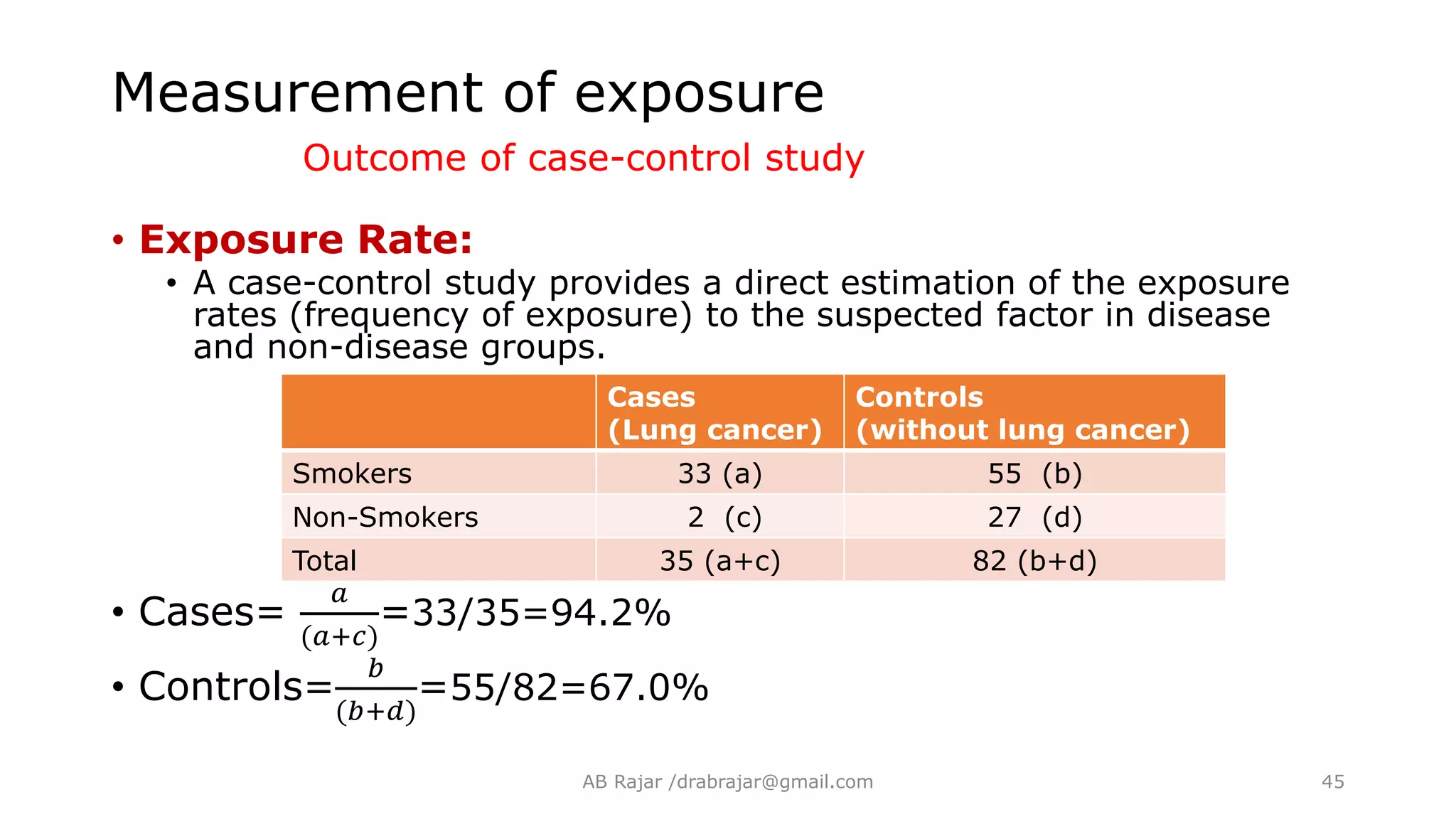
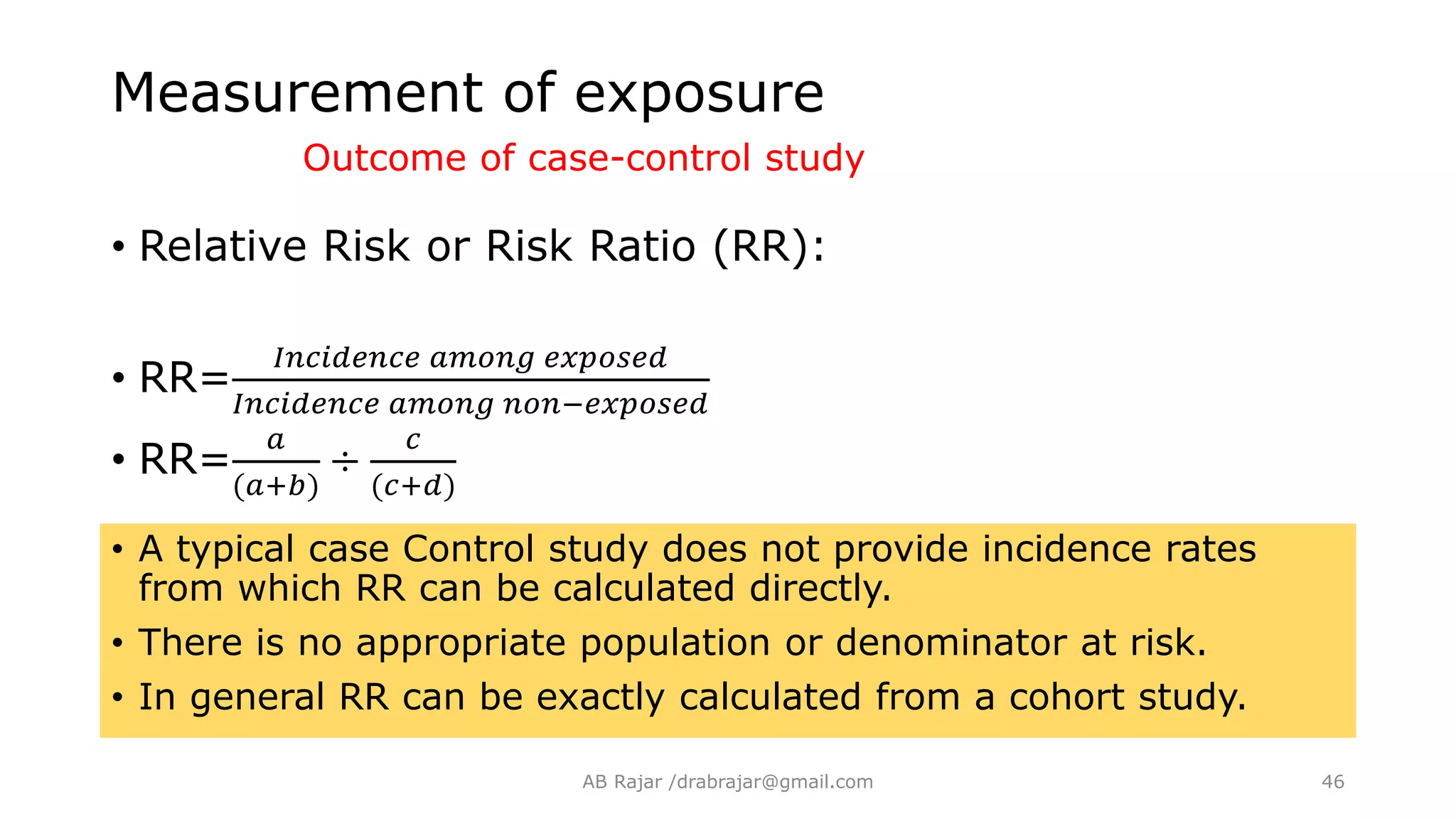
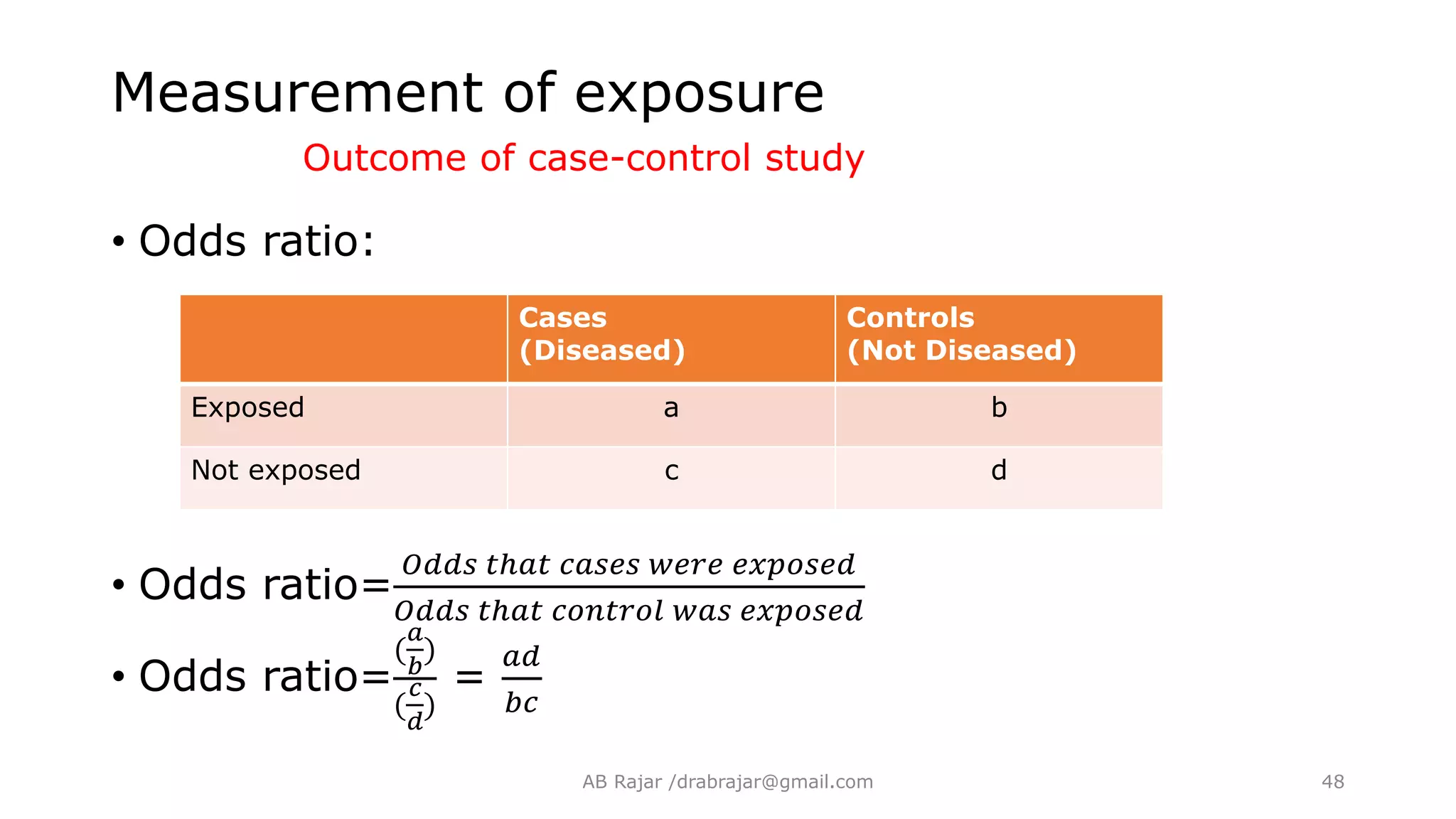
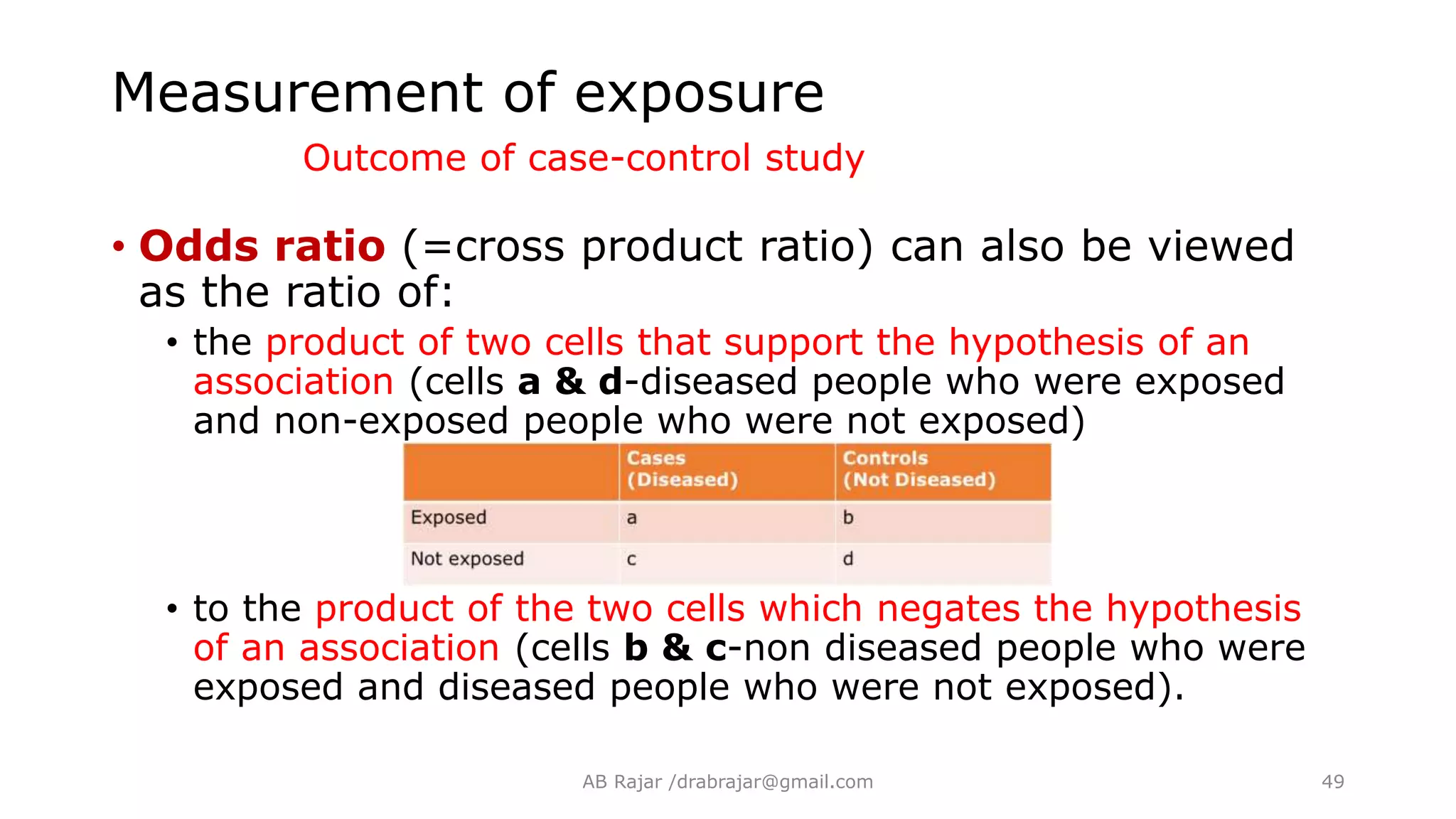
Explains how exposure is assessed in case-control studies, including methods like interviews and questionnaires, and detailing odds ratios.
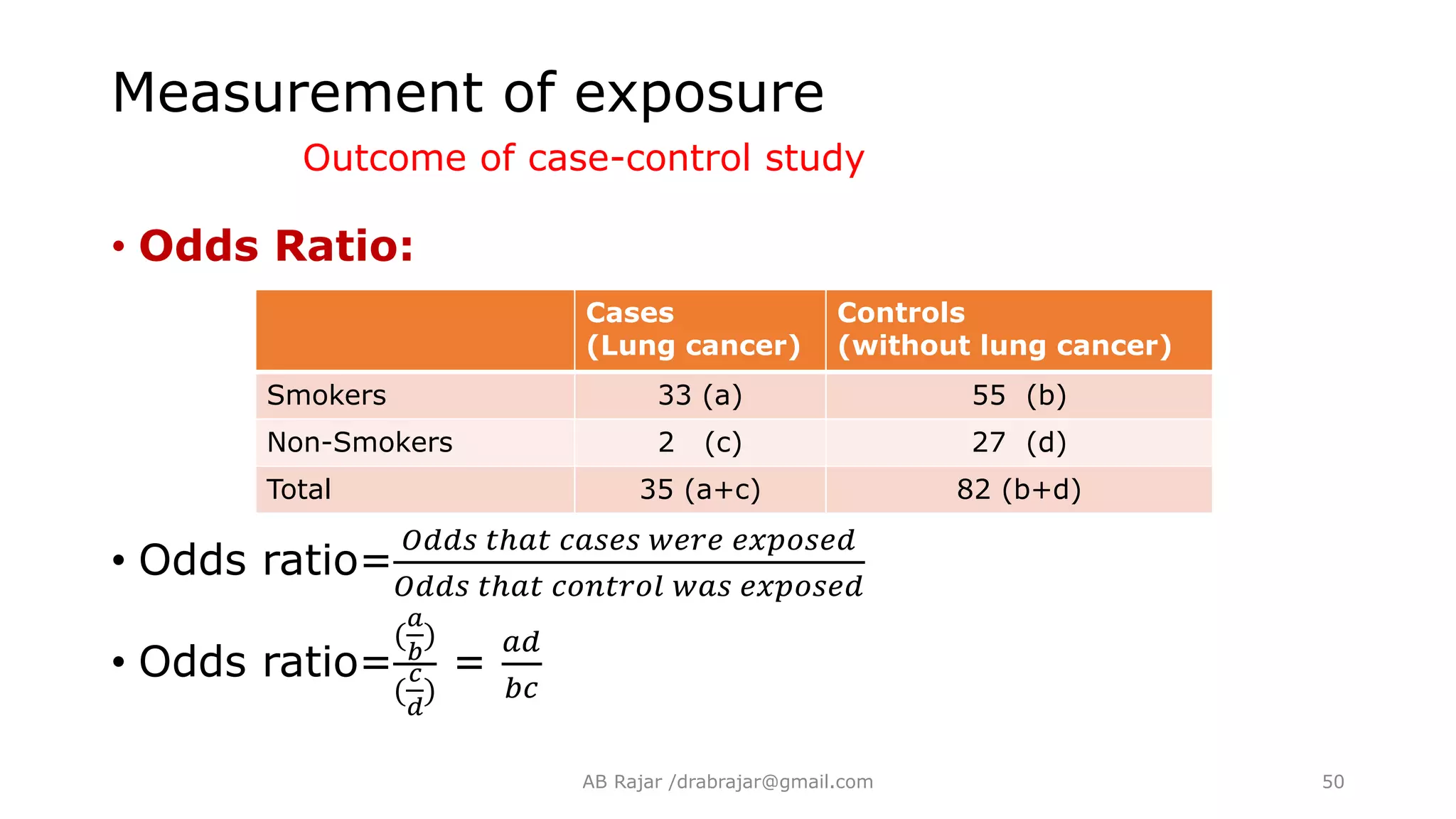
Analyzing exposure data, calculating odds ratios, and the implications of different odds ratio values in establishing risk factors.
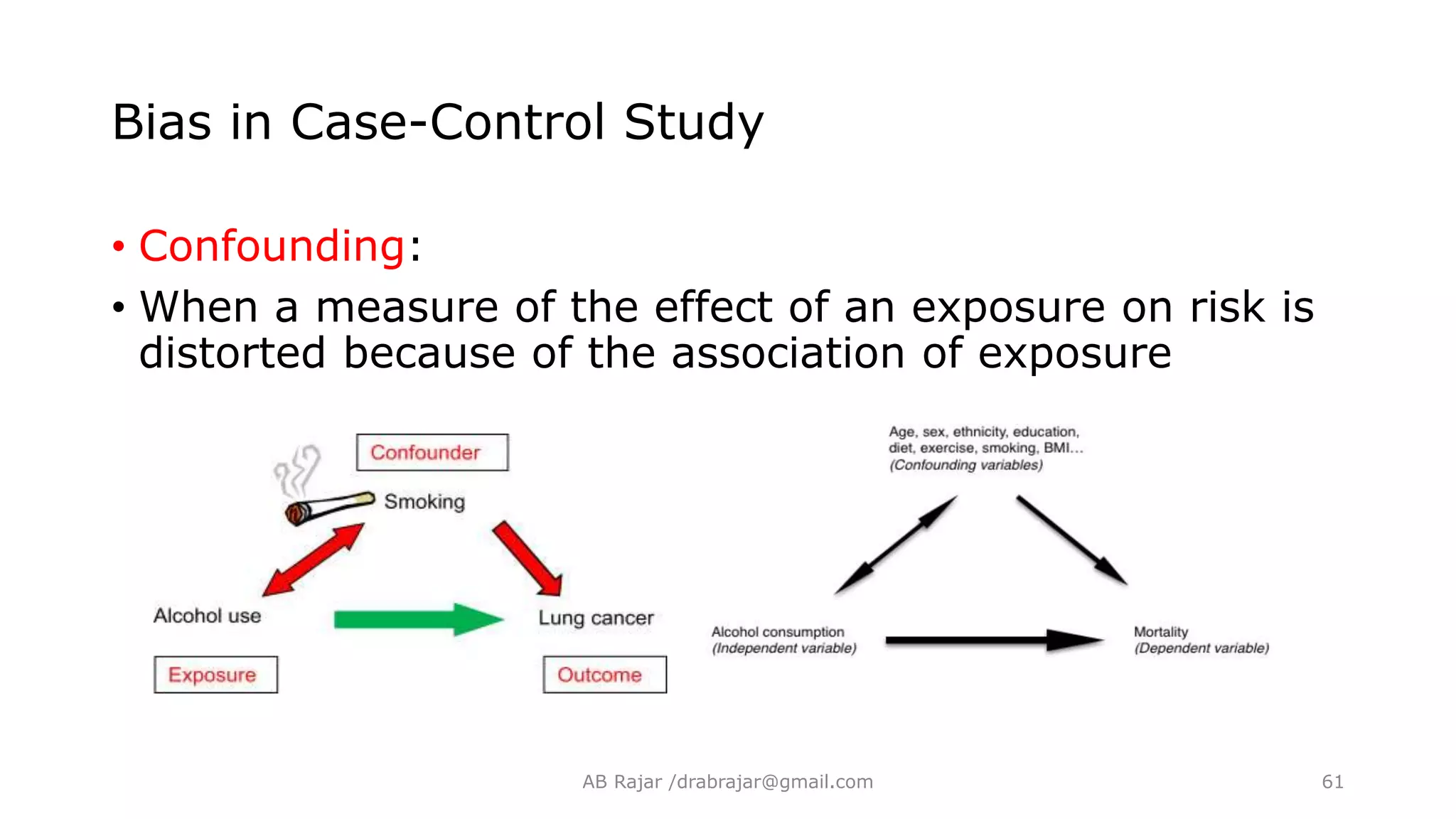
Identifying potential biases (selection, information, confounding) impacting study results and emphasizing their importance in study design.
Outlines the benefits and limitations of case-control studies, including aspects like cost, efficiency, and susceptibility to bias.
Engages participants in assessing understanding through relevant multiple-choice questions related to the topics discussed.
Conclusion of the presentation, thanking attendees and inviting further questions.























































































