Downloaded 3,745 times

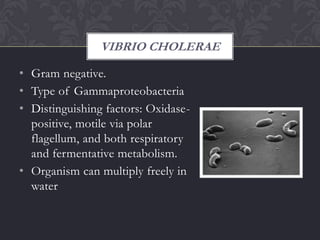
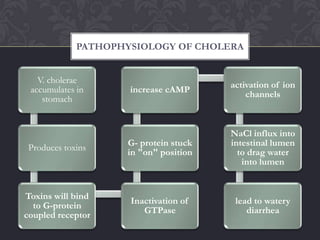

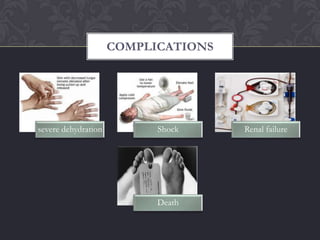

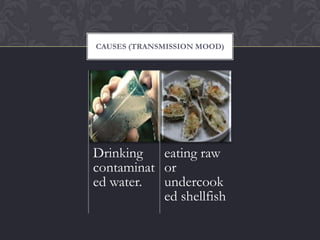

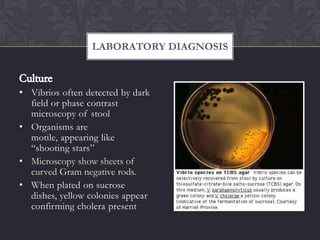









Cholera is an acute diarrheal illness caused by the bacteria Vibrio cholerae. It spreads when the feces of an infected person come into contact with food or water. Symptoms include profuse watery diarrhea, vomiting, and leg cramps. Treatment focuses on oral rehydration salts or intravenous fluids for severe cases. Prevention emphasizes basic hygiene, provision of safe water and sanitation, and vaccination programs. With prompt treatment, mortality rates from cholera can be reduced to about 1%.
































































































