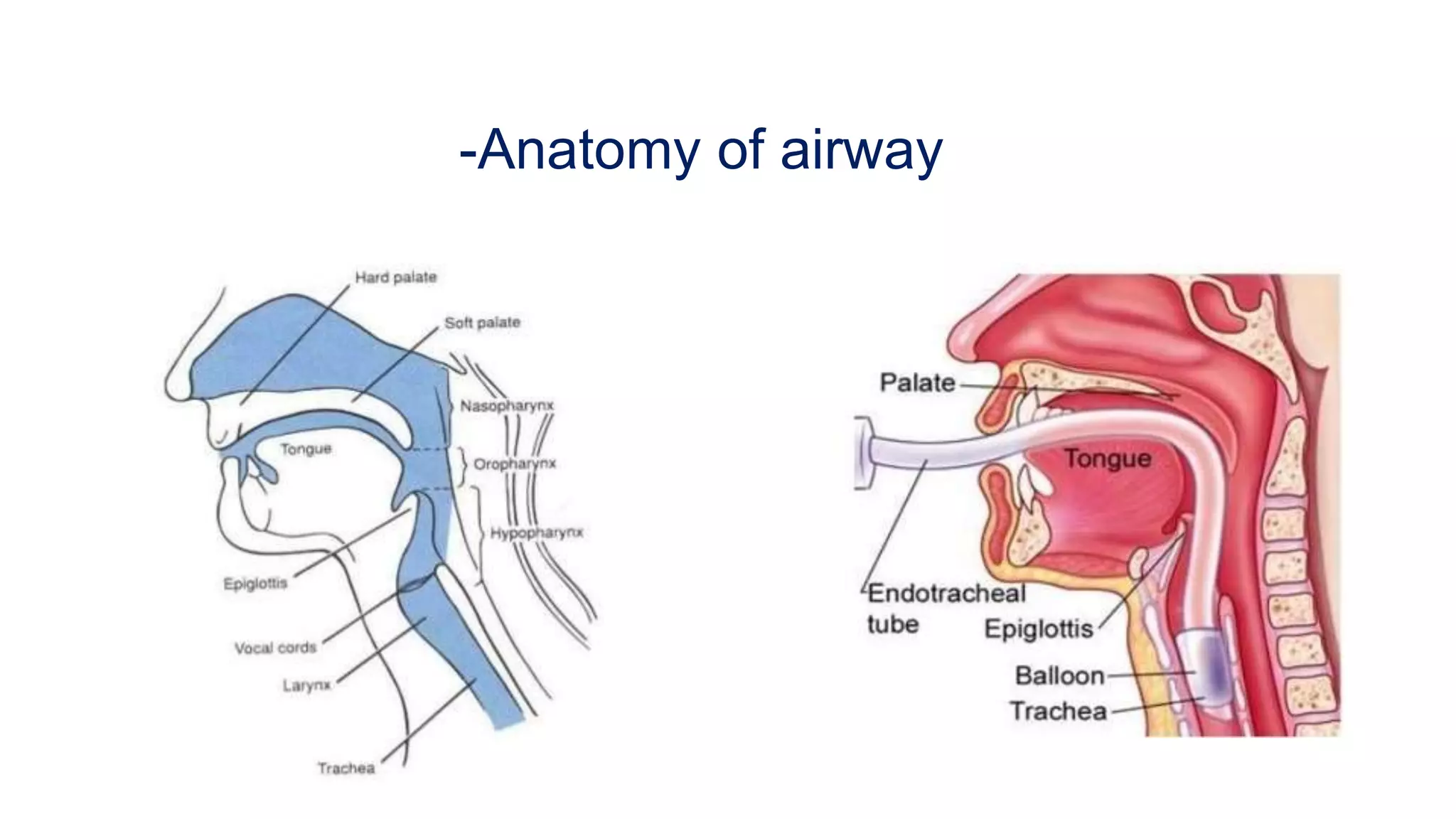
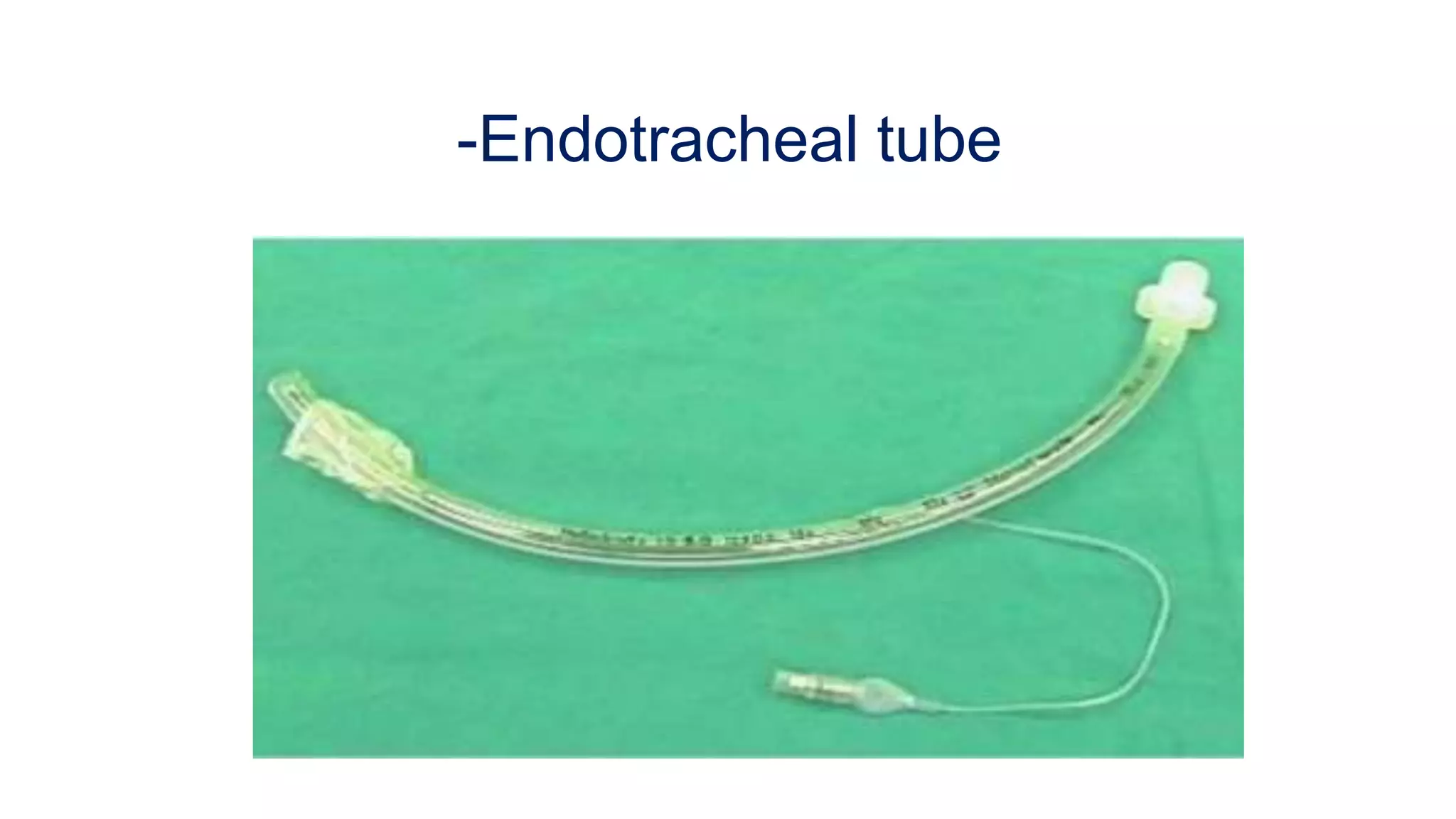
This document discusses endotracheal tubes and intubation. It covers indications for intubation including airway protection, optimizing gas exchange, decreasing metabolic demand, and reducing work of breathing. Conditions associated with difficult intubation are described such as congenital anomalies, infections, tumors, and injuries. Airway assessment techniques like mallampati classification, laryngoscopy view, and thyromental distance are explained. Equipment for intubation and appropriate endotracheal tube sizes are listed. The technique of endotracheal intubation is outlined in steps. Confirmation of proper tube placement is also discussed.