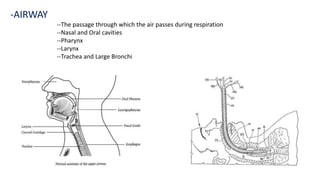
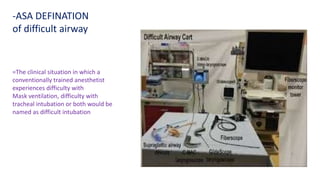
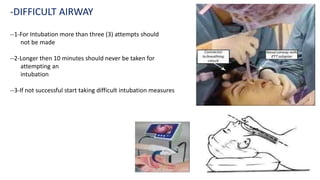
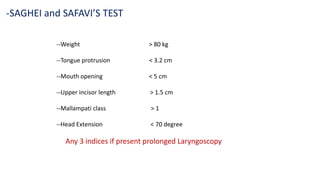
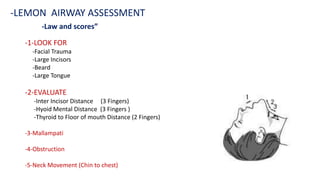
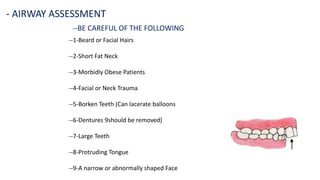
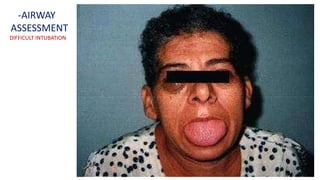
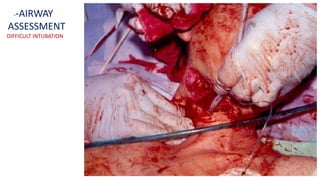
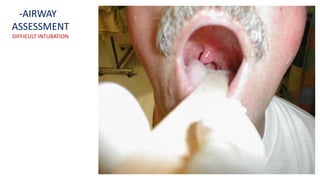
This document discusses airway assessment and difficult airways. It outlines various predictors of difficult airways like obesity, short neck, and facial hair. It describes tests to evaluate the airway like thyromental distance, inter-incisor gap, and Mallampati grading. The document emphasizes the importance of a thorough airway assessment prior to intubation to identify potential difficulties and prepare appropriate management strategies for difficult intubations.


















































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)









