








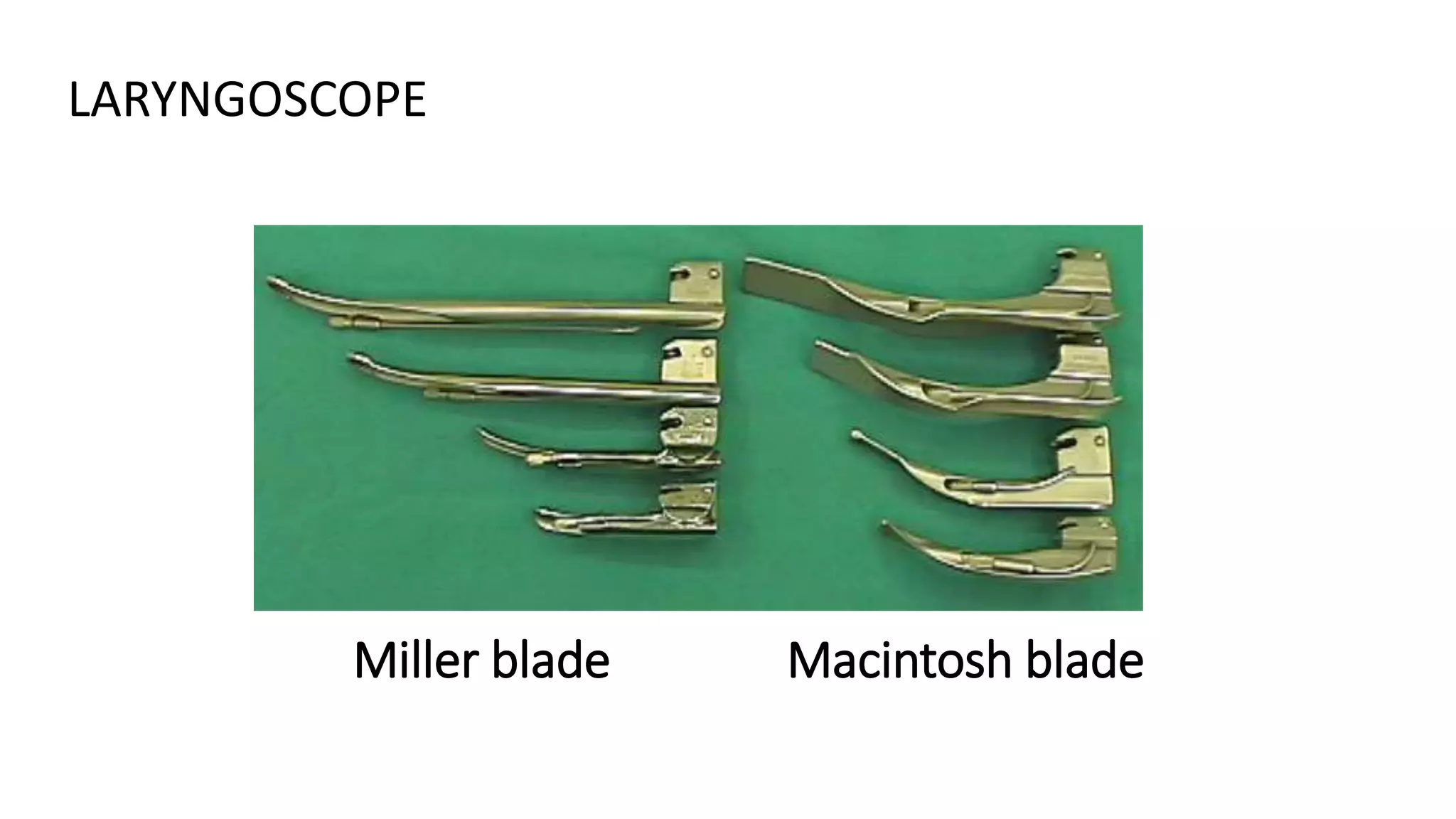



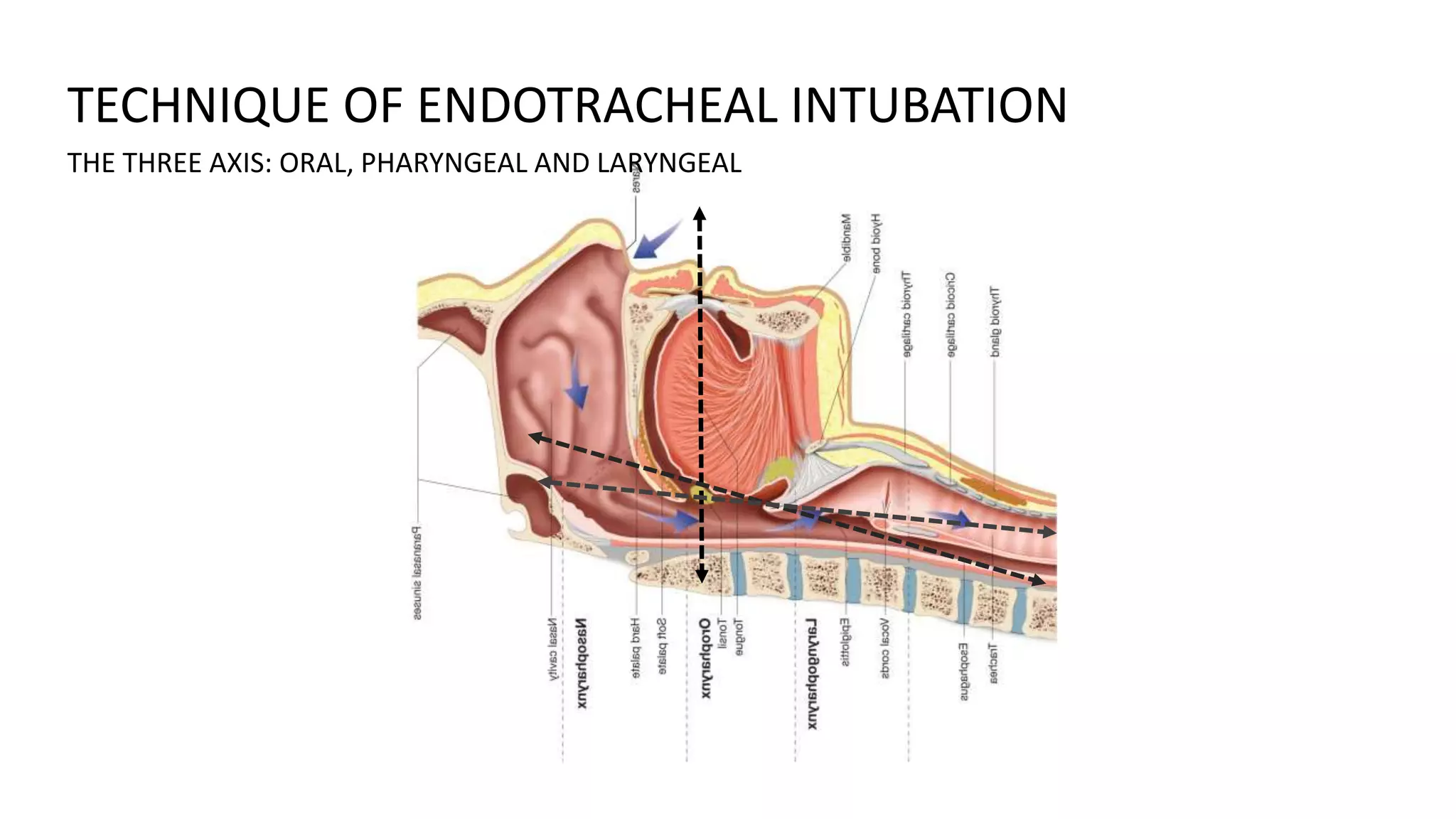





This document discusses endrotracheal intubation including indications, anatomy, equipment, technique, and confirmation of proper tube placement. Key points include intubation is indicated for airway protection, optimizing gas exchange, decreasing metabolic demand. Proper equipment includes laryngoscope, endotracheal tubes, airways. Technique involves aligning three axes of oral, pharyngeal and laryngeal, lifting epiglottis to view cords, passing tube through cords. Placement is confirmed visually and by auscultation of breath sounds over lungs.























































































