Download as PDF, PPTX







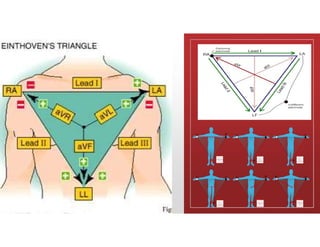
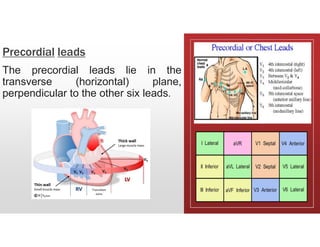

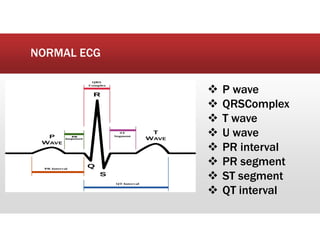
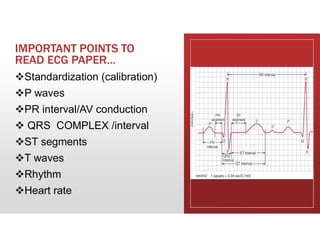
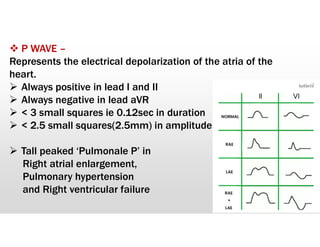
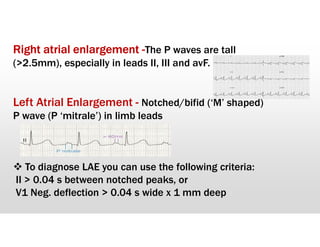
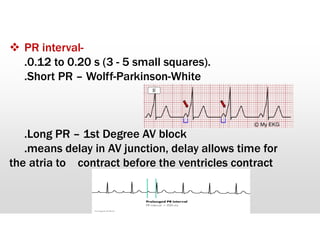
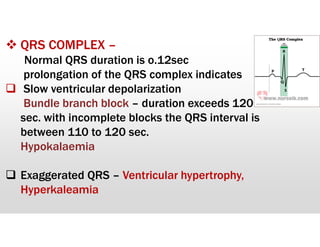
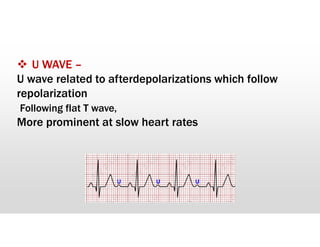
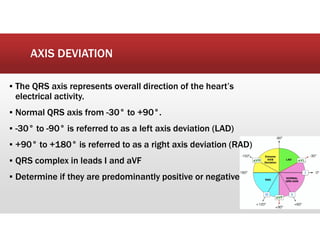
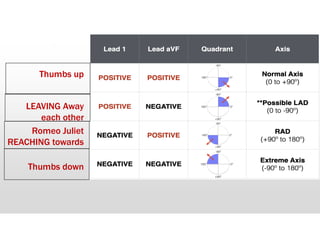
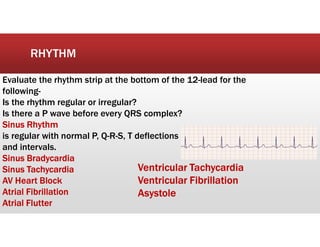
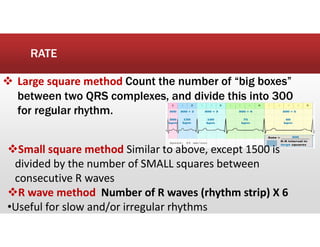


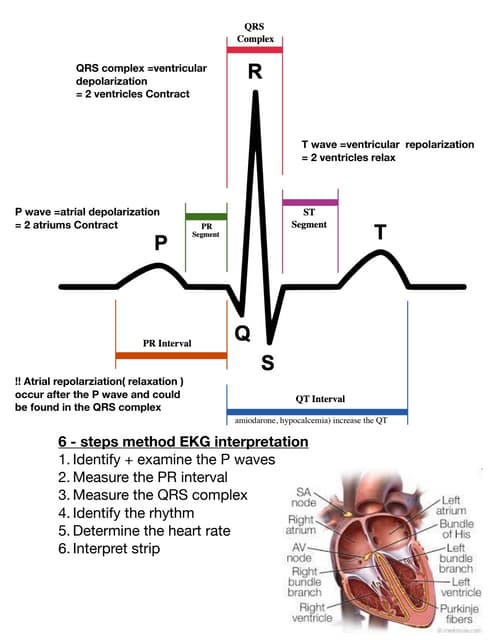
This document provides an overview of electrocardiography (ECG) and how to interpret an ECG. It discusses the history and importance of ECG, the conduction system of the heart, how ECG leads work, what a normal ECG waveform looks like, how to evaluate rhythm and rate, and how to identify common abnormalities. Key aspects of a normal ECG that are described include the P wave, PR interval, QRS complex, ST segment, T wave, and QT interval. Common abnormalities that can be identified on an ECG include arrhythmias, myocardial infarction, chamber enlargement, and electrolyte imbalances.