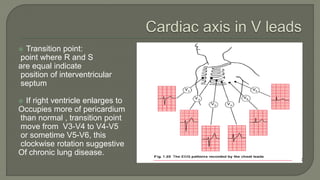
The document discusses the electrocardiogram (ECG), which represents the electrical events of the cardiac cycle, providing insights into conditions like arrhythmias and myocardial ischemia. It details the heart's electrical conduction system, including the roles of the SA node and AV node, as well as the interpretation of various waveforms and intervals on the ECG. Additionally, it covers the significance of cardiac axis deviations and the influence of cardiac structure and health on the electrocardiographic readings.





















































![PT management in CKD [Renal Rehabilitation].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/ptmanagementinckdrenalrehabilitation-220727071020-ee721238-thumbnail.jpg?width=640&height=640&fit=bounds)





































