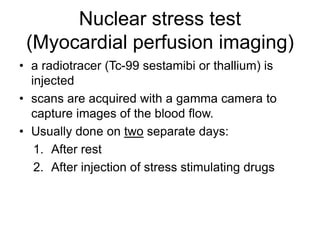
Cardiac stress tests are used to diagnose coronary artery disease by assessing how the heart responds to induced stress. Stress can be induced through exercise on a treadmill or stationary bike or through pharmacological agents. The test measures for changes in electrocardiography, echocardiography, or nuclear imaging before and after stress is applied to detect any signs of ischemia. Stress tests are indicated for diagnosing chest pain, prior heart attacks, or post-revascularization and help evaluate the heart's response to physical or drug stimulation.




























![Stresstesting housestaffdidactic_10092014[1]](https://cdn.slidesharecdn.com/ss_thumbnails/stress20testinghousestaff20didactic100920141-141013101956-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Stress%20 testing housestaff%20didactic_10092014[1]](https://cdn.slidesharecdn.com/ss_thumbnails/stress20testinghousestaff20didactic100920141-141013101524-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)


































![谷歌留痕技术 [ 𝙩𝙤𝙥 𝟮𝟯𝟯. 𝙘 𝙤𝙢 ]](https://cdn.slidesharecdn.com/ss_thumbnails/top233-260130174328-3833018c-thumbnail.jpg?width=640&height=640&fit=bounds)

