Downloaded 31 times
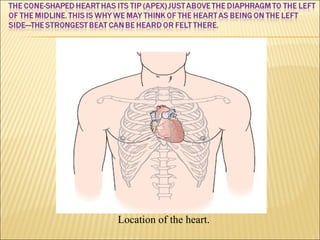
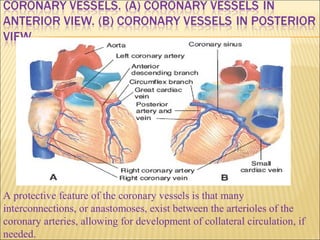
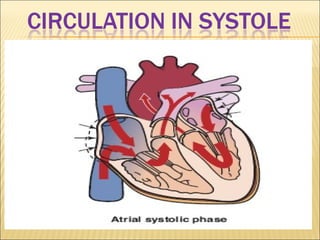
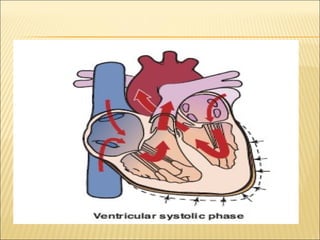
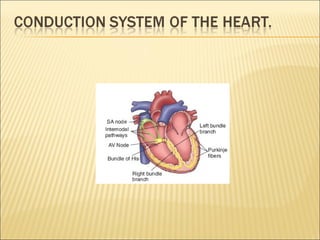
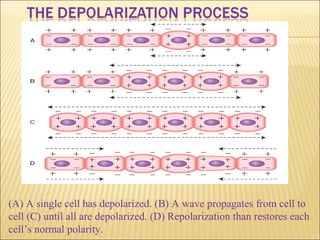
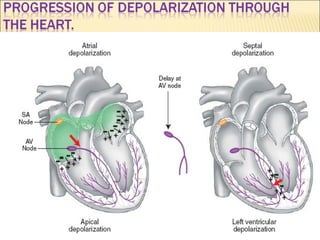
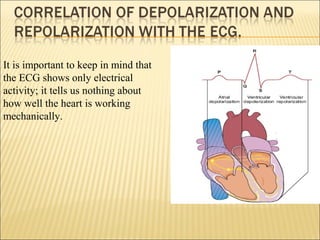
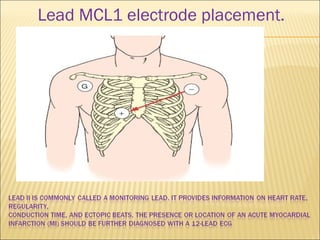
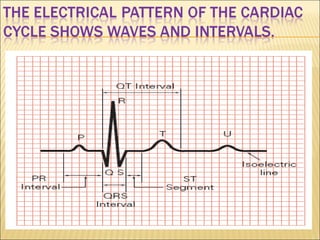
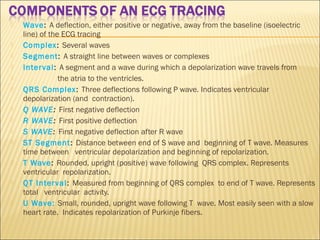


The document provides information about ECG basics. It discusses: 1) The location of the heart and the protective feature of coronary vessels which allow for collateral circulation. 2) How an ECG works by showing the electrical activity of a single cell depolarizing and propagating in a wave through the heart until repolarization restores the cells. 3) An ECG shows only electrical activity and not mechanical heart function. It provides definitions of key waves, complexes, intervals and segments seen on an ECG tracing.




















































![Shadechapter02.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter02-150421101545-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)








![ECG [electrocardiogram].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/ecgelectrocardiogram-220416062706-thumbnail.jpg?width=640&height=640&fit=bounds)