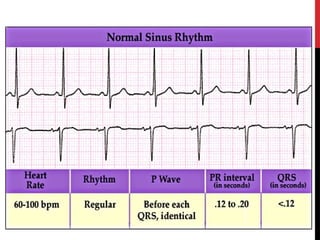
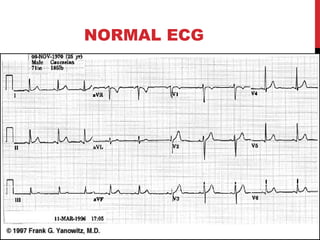
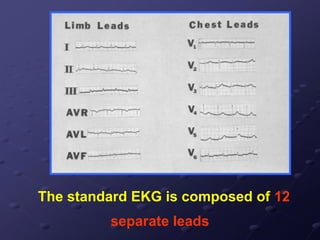
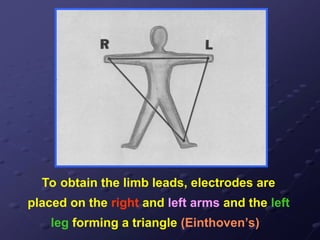
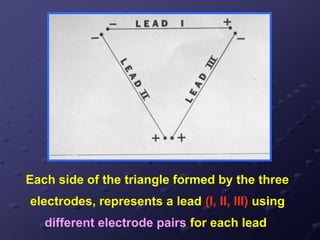
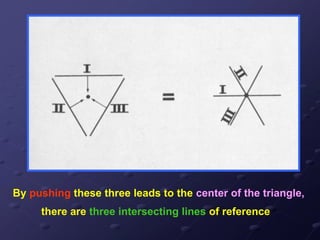
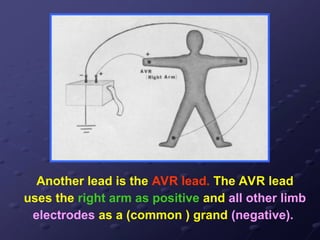
The document provides a detailed overview of the cardiac cycle, its physiological properties, and the principles of electrocardiography (ECG). It describes the electrical and mechanical phases of the cardiac cycle, components of ECG, and how to interpret the data it provides regarding heart function. Additionally, it outlines the types of ECG monitoring, lead configurations, and methods for calculating heart rate.





















![ECG [electrocardiogram].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/ecgelectrocardiogram-220416062706-thumbnail.jpg?width=640&height=640&fit=bounds)





























