Download as PPSX, PPTX


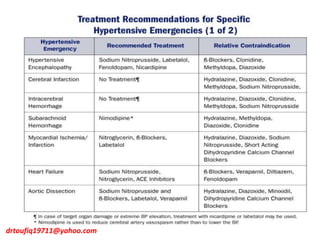
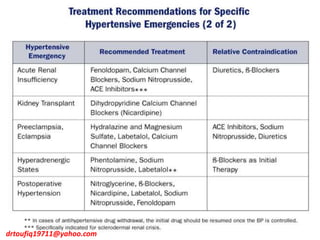
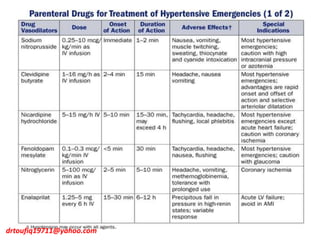
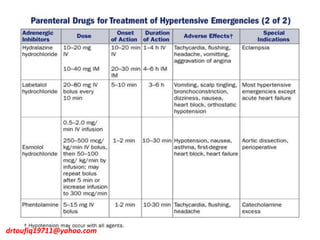
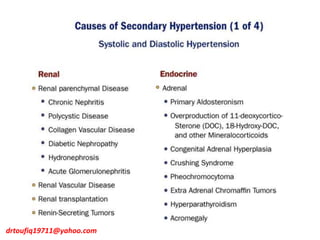
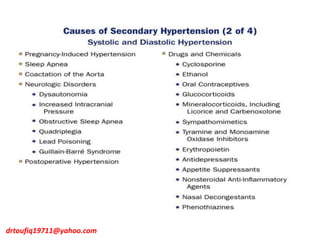
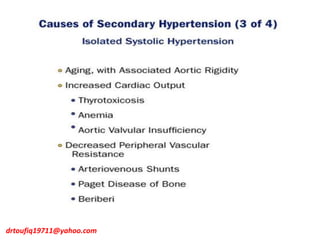
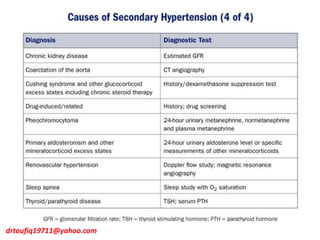
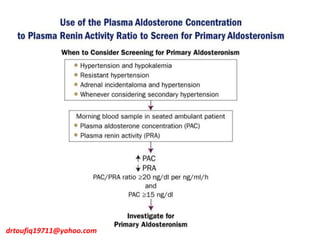
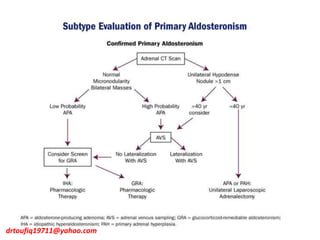
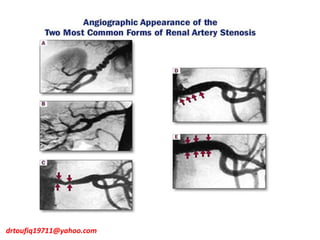
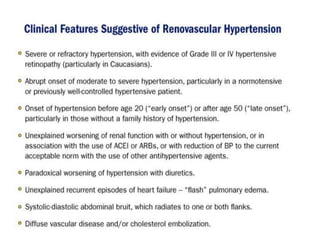
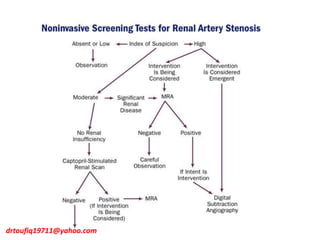
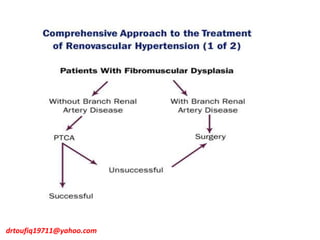
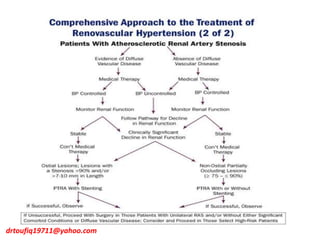
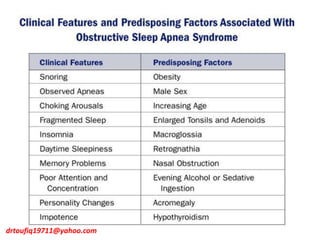


The document discusses the management of hypertension in specific situations, differentiating between hypertensive urgency and hypertensive emergency. It highlights the significance of secondary hypertension causes, particularly primary aldosteronism and renovascular hypertension, with specific diagnostic and management strategies for each. Additionally, it covers obstructive sleep apnea's impact on hypertension and the importance of sleep testing for accurate diagnosis.











































































































