Downloaded 140 times
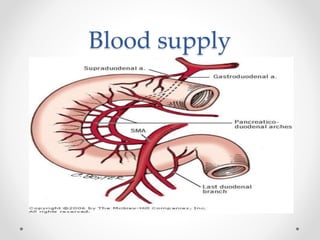
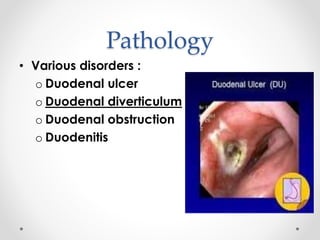
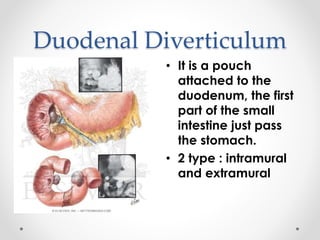
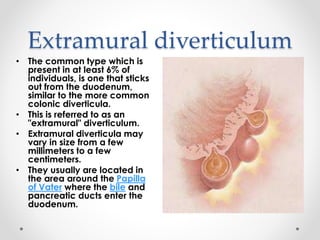

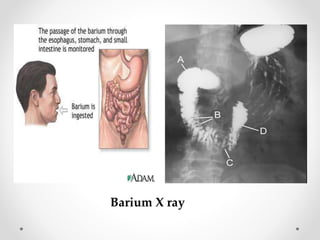
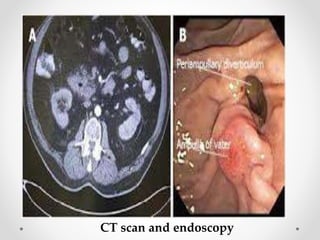
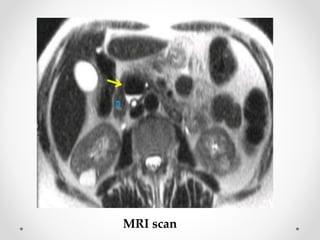
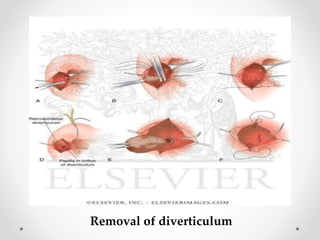
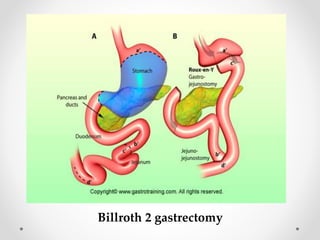


The duodenum is the C-shaped, initial part of the small intestine that is continuous with the stomach. Duodenal diverticula are pouches that can protrude either outside (extramural) or inside (intramural) the duodenum wall. Extramural diverticula are more common, located near the bile duct entrance, and their cause is not fully known. Most duodenal diverticula are asymptomatic, but some people experience abdominal pain, nausea, or jaundice. Complications can include gallstones, pancreatitis, or bile duct inflammation. Diagnosis involves imaging like barium X-rays, endoscopy, CT scans, or MRI. Treatment of symptomatic diverticula


































































![diverticular disease [تم حفظه تلقائيا] 3.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/diverticulardisease3-240512203054-95042ff3-thumbnail.jpg?width=640&height=640&fit=bounds)








































