DEVELOPMENT OF GIT
ANDMALROTATION
MODERATOR: Dr.K.SAMBASIVA RAO MDRD
HOD AND PROFESSOR
PRESENTER:Dr.SNEHA
PGY1
2.
DEVELOPMENT OF GIT
•EMBRYONIC FOLDING
- Development of gut tube
- Development of peritoneum
• FOREGUT , MIDGUT , HINDGUT
-Components
-Vascular supply
-Mesenteries
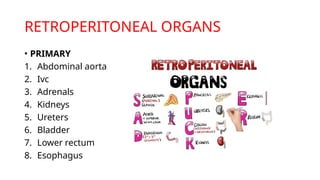
• RETROPERITONEAL ORGANS
• MALROTATION
3.
FORMATION OF PRIMITIVEGUT TUBE
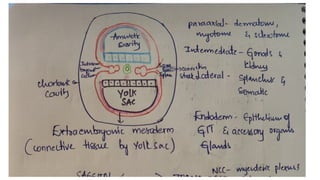
• The gut tube is formed from endoderm lining the yolk sac
which is enveloped by the developing coelom as the result
of cranial and caudal folding.
• During folding , somatic mesoderm is applied to the body
wall to give rise to the parietal peritoneum.
• Visceral (splanchnic) mesoderm wraps around the gut tube
to form the mesenteries that suspend the gut tube within
the body cavity.
• The mesoderm immediately associated with the
endodermal tube also contributes to most of the gut tube.
7.
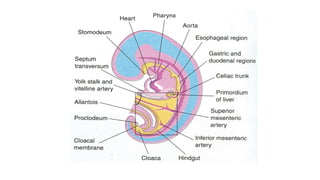
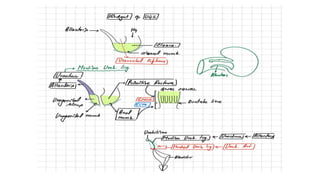
DEFINITIVE SUBDIVISIONS OFTHE GUT
TUBE
• Within the abdominal cavity, the gut is definitively divided
into foregut, midgut, and hindgut.
• BASED ON THE ARTERIAL SUPPLY:-
• Foregut derivatives in the abdomen are supplied by
branches of the celiac artery.
• Midgut derivatives are supplied by branches of the superior
mesenteric artery.
• Hindgut derivatives are supplied by branches of the inferior
mesenteric artery.
8.
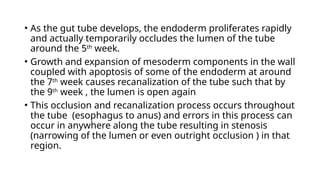
• As thegut tube develops, the endoderm proliferates rapidly
and actually temporarily occludes the lumen of the tube
around the 5th
week.
• Growth and expansion of mesoderm components in the wall
coupled with apoptosis of some of the endoderm at around
the 7th
week causes recanalization of the tube such that by
the 9th
week , the lumen is open again
• This occlusion and recanalization process occurs throughout
the tube (esophagus to anus) and errors in this process can
occur in anywhere along the tube resulting in stenosis
(narrowing of the lumen or even outright occlusion ) in that
region.
11.
DERIVATIVES OF FOREGUT
•Trachea and respiratory tract
• Lungs
• Esophagus
• Stomach
• Liver gall bladder and bile ducts
• Pancreas (dorsal and ventral)
• Upper duodenum
• Mesentery [dorsal and ventral mesogastrium]
12.
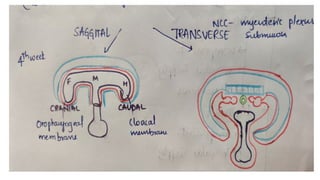
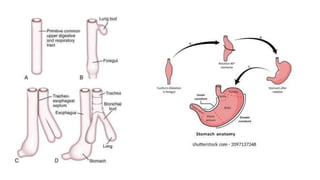
ESOPHAGUS AND TRACHEA:-Theregion of foregut just
caudal to the pharynx develops two longitudinal ridges
called the tracheoesophageal folds that divide the tube
ventrally into trachea (and subsequent lung buds), and
dorsally into the esophagus.
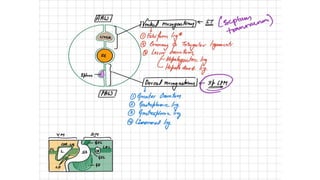
STOMACH :- It appears as a fusiform dilation of the foregut
endoderm which undergoes a 90 rotation such that the left
◦
side moves ventrally and the right moves dorsally [the vagus
nerve follows this rotation which is how the left vagus
becomes anterior and the right vagus becomes posterior].
13.
-differential growth onthe left and right side establishes the
greater and lesser curvatures respectively; craniocaudal
rotation tips the pylorus superiorly
-dorsal and ventral mesenteries of the stomach are
retained to become the greater and lesser omentum.
15.
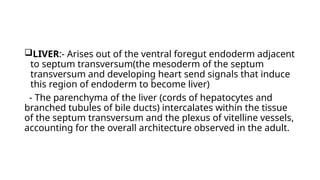
LIVER:- Arises outof the ventral foregut endoderm adjacent
to septum transversum(the mesoderm of the septum
transversum and developing heart send signals that induce
this region of endoderm to become liver)
- The parenchyma of the liver (cords of hepatocytes and
branched tubules of bile ducts) intercalates within the tissue
of the septum transversum and the plexus of vitelline vessels,
accounting for the overall architecture observed in the adult.
16.
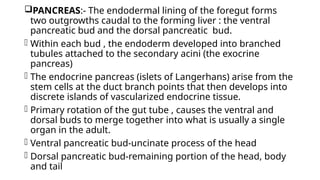
PANCREAS:- The endodermallining of the foregut forms
two outgrowths caudal to the forming liver : the ventral
pancreatic bud and the dorsal pancreatic bud.
- Within each bud , the endoderm developed into branched
tubules attached to the secondary acini (the exocrine
pancreas)
- The endocrine pancreas (islets of Langerhans) arise from the
stem cells at the duct branch points that then develops into
discrete islands of vascularized endocrine tissue.
- Primary rotation of the gut tube , causes the ventral and
dorsal buds to merge together into what is usually a single
organ in the adult.
- Ventral pancreatic bud-uncinate process of the head
- Dorsal pancreatic bud-remaining portion of the head, body
and tail
17.
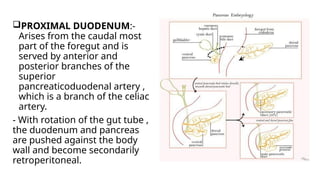
PROXIMAL DUODENUM:-
Arises fromthe caudal most
part of the foregut and is
served by anterior and
posterior branches of the
superior
pancreaticoduodenal artery ,
which is a branch of the celiac
artery.
- With rotation of the gut tube ,
the duodenum and pancreas
are pushed against the body
wall and become secondarily
retroperitoneal.
DISTAL DUODENUM:- Distalor lower duodenum arises
from the cranial most portion of the midgut and is served
by anterior and posterior branches of the inferior
pancreaticoduodenal artery, branch of SMA.
JEJUNUM, ILEUM PORTION OF LARGE INTESTINE FROM
MIDGUT:- Midgut elongates rapidly beyond the capacity of
the embryonic abdominal cavity and thus forms a u shaped
loop that herniates into the umbilicus and is oriented
parallel to axis of the embryo such that there is an upper or
cranial loop[jejunum and upper pat of ileum] and a lower or
caudal loop.
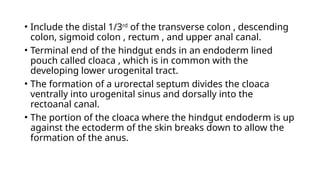
• Include thedistal 1/3rd
of the transverse colon , descending
colon, sigmoid colon , rectum , and upper anal canal.
• Terminal end of the hindgut ends in an endoderm lined
pouch called cloaca , which is in common with the
developing lower urogenital tract.
• The formation of a urorectal septum divides the cloaca
ventrally into urogenital sinus and dorsally into the
rectoanal canal.
• The portion of the cloaca where the hindgut endoderm is up
against the ectoderm of the skin breaks down to allow the
formation of the anus.
• SECONDARY
1. 2,3,4TH PART OF THE DUODENUM
2. ASCENDING COLON
3. DESCENDING COLON
4. HEAD AND BODY OF PANCREAS
These organs connects to the posterior wall through
adventitia.
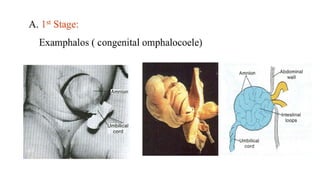
1]OMPHALOCELE
• A/K/A EXOMPHALOS, are congenital midline abdominal
wall defects at the base of the umbilical cord insertion, with
herniation of gut [or occasionally other structures ] out of
the fetal abdomen.
• USG:- multiple bowel loops (and on occasion liver) herniate
into a membrane-covered defect (i.e. not free-flowing) and
are usually seen as hyperechogenic content (non-fluid filled
bowel)
• the umbilical cord insertion is directly into the omphalocele
32.
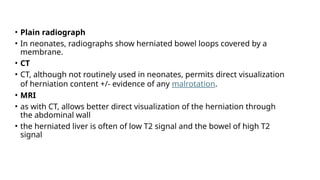
• Plain radiograph
•In neonates, radiographs show herniated bowel loops covered by a
membrane.
• CT
• CT, although not routinely used in neonates, permits direct visualization
of herniation content +/- evidence of any malrotation.
• MRI
• as with CT, allows better direct visualization of the herniation through
the abdominal wall
• the herniated liver is often of low T2 signal and the bowel of high T2
signal
33.
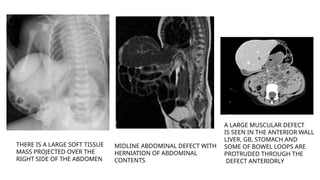
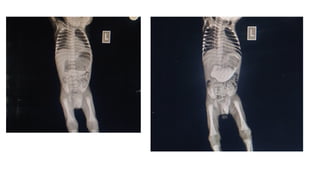
THERE IS ALARGE SOFT TISSUE
MASS PROJECTED OVER THE
RIGHT SIDE OF THE ABDOMEN
MIDLINE ABDOMINAL DEFECT WITH
HERNIATION OF ABDOMINAL
CONTENTS
A LARGE MUSCULAR DEFECT
IS SEEN IN THE ANTERIOR WALL
LIVER, GB, STOMACH AND
SOME OF BOWEL LOOPS ARE
PROTRUDED THROUGH THE
DEFECT ANTERIORLY
34.
2]GASTROSCHISIS
• Extra-abdominal herniationof fetal or neonatal bowel loops (and
occasionally portions of the stomach , liver , and/or gall bladder)
into the amniotic cavity through a para-umbilical anterior
abdominal wall defect.
• USG:-The herniated content is towards the right side of the
umbilical cord in most cases; color Doppler may be useful to locate
the cord in relation to the herniation. This causes the fetal
abdominal circumference to be smaller than expected for
gestation age. The herniated bowel often appears free-floating
rather than contained. The herniated bowel wall can be thickened
due to edema.
• There can be either accompanying oligohydramnios or
polyhydramnios as ancillary sonographic sonographic features.
36.
THERE IS HERNIATIONOF SMALL BOWEL LOOPS
THROUGH A RIGHT PARAUMBILICAL ABDOMINAL
WALL DEFECT. AIR IS SEEN IN THE STOMACH. THERE
IS NO SOLID ORGAN HERNIATION EVIDENT
THERE IA AN ANTERIOR ABDOMINAL WALL DEFECT
WITH PROTRUSION OF THE BOWEL LOOPS OUT
THE ABDOMINAL CAVITY WITHOUT ANY COVERING
37.
3]MECKEL DIVERTICULUM
• Remnantof the vitelline duct, which connects the yolk sac to the
midgut through the umbilical cord. This duct is typically
obliterated by the 5th
to 8th
week of gestation.
• Fluoroscopy
• Small bowel enemas have sometimes been used for the diagnosis
in some centers, although a precise technique is required if the
diagnosis is to be excluded with any degree of certainty 4
.
• Ultrasound
• Usually of limited use in the diagnosis of an uncomplicated
Meckel diverticulum. Ultrasound may show a blind-ending
peristaltic loop connected to the small bowel - it may have a
multi-layered appearance of the wall.
38.
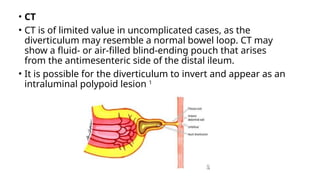
• CT
• CTis of limited value in uncomplicated cases, as the
diverticulum may resemble a normal bowel loop. CT may
show a fluid- or air-filled blind-ending pouch that arises
from the antimesenteric side of the distal ileum.
• It is possible for the diverticulum to invert and appear as an
intraluminal polypoid lesion 1
39.
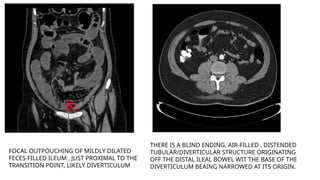
FOCAL OUTPOUCHING OFMILDLY DILATED
FECES-FILLED ILEUM , JUST PROXIMAL TO THE
TRANSITION POINT, LIKELY DIVERTICULUM
THERE IS A BLIND ENDING, AIR-FILLED , DISTENDED
TUBULAR/DIVERTICULAR STRUCTURE ORIGINATING
OFF THE DISTAL ILEAL BOWEL WIT THE BASE OF THE
DIVERTICULUM BEAING NARROWED AT ITS ORIGIN.
40.
4]MALROTATION
• In thedeveloping embryo growth of the bowel requires herniation
into the omphalomesenteric sac.
In the tenth week of gestation the bowel returns to the abdominal
cavity.
• This return is accompanied by a counterclockwise rotation of the
midgut to achieve its final position with the ligament of Treitz in the
left upper quadrant and the caecum in the right lower quadrant,
suspended from a long mesentery.
• Malrotation arises when the rotation is arrested or even reversed.
As a result the bowel has an abnormal position, the mesentery is
short and peritoneal bands, called Ladd's bands, may cross from the
caecum to the liver or to the anterior abdominal wall.
41.
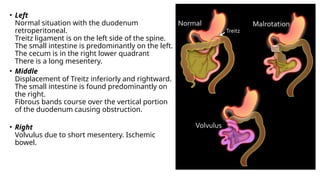
• Left
Normal situationwith the duodenum
retroperitoneal.
Treitz ligament is on the left side of the spine.
The small intestine is predominantly on the left.
The cecum is in the right lower quadrant
There is a long mesentery.
• Middle
Displacement of Treitz inferiorly and rightward.
The small intestine is found predominantly on
the right.
Fibrous bands course over the vertical portion
of the duodenum causing obstruction.
• Right
Volvulus due to short mesentery. Ischemic
bowel.
42.
• The malrotationwill become symptomatic only when a
volvulus occurs due to the short mesentery or when the
Ladd's band obstruct the duodenum
• Both presentations are most common in the neonatal
period.
• However sometimes it can also present later in life, for
example when the volvulus is intermittent or when the
Ladd's bands create relatively little obstruction.
• Acute volvulus is a life-threatening presentation and
requires prompt surgical intervention.
43.
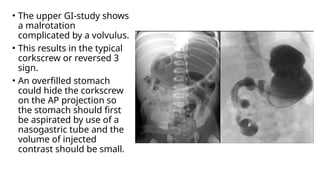
• The upperGI-study shows
a malrotation
complicated by a volvulus.
• This results in the typical
corkscrew or reversed 3
sign.
• An overfilled stomach
could hide the corkscrew
on the AP projection so
the stomach should first
be aspirated by use of a
nasogastric tube and the
volume of injected
contrast should be small.
44.
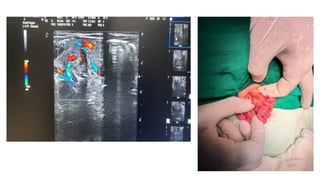
• Sometimes amalrotation can be suspected when
on ultrasound the superior mesenteric artery is
seen to lie to the right of the superior mesenteric
vein.
• This sign however is neither specific nor sensitive
and should not be used when asked to investigate
for suspected malrotation without a volvulus.
• An abnormal location of ligament of Treitz on an
upper GI series is the gold standard for malrotation.
45.
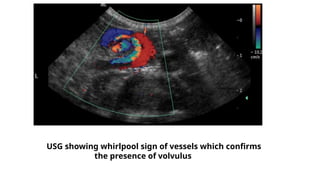
• In caseof a volvulus the child is acutely sick and ultrasound
is often the modality of choice.
• This will show a whirlpool sign of the vessels which confirms
the presence of a volvulus.
• The corkscrew sign of the bowel on the upper GI is
equivalent.
Once a volvulus is diagnosed on ultrasound, the child
should go straight to the operating room and no more time
should be lost on further imaging.
5] DUODENAL ATRESIA/STENOSIS
•Duodenal atresia results from a congenital malformation of
the duodenum and requires prompt correction in the
neonatal period. It is considered to be one of the
commonest causes of fetal bowel obstruction.
• Plain radiograph
• Abdominal radiographs may classically show a
double bubble sign with gas filled distended stomach and
duodenum with an absence of distal gas. A similar
appearance (either filled with fluid or gas) can be seen in
other modalities.
52.
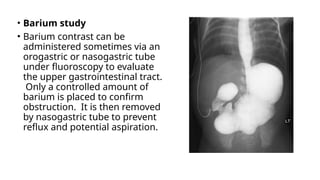
• Barium study
•Barium contrast can be
administered sometimes via an
orogastric or nasogastric tube
under fluoroscopy to evaluate
the upper gastrointestinal tract.
Only a controlled amount of
barium is placed to confirm
obstruction. It is then removed
by nasogastric tube to prevent
reflux and potential aspiration.
53.
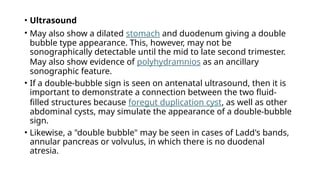
• Ultrasound
• Mayalso show a dilated stomach and duodenum giving a double
bubble type appearance. This, however, may not be
sonographically detectable until the mid to late second trimester.
May also show evidence of polyhydramnios as an ancillary
sonographic feature.
• If a double-bubble sign is seen on antenatal ultrasound, then it is
important to demonstrate a connection between the two fluid-
filled structures because foregut duplication cyst, as well as other
abdominal cysts, may simulate the appearance of a double-bubble
sign.
• Likewise, a "double bubble" may be seen in cases of Ladd's bands,
annular pancreas or volvulus, in which there is no duodenal
atresia.
54.
Gaseous distension ofstomach and
proximal duodenum with absence of
bowel gas distally giving the classical
appearance of double bubble sign,
compatible with duodenal atresia.
Antenatal ultrasound showing increased liquor amnii
(polyhydramnios) with two communicating cystic
structures in upper abdomen of the fetus suggestive
of double bubble sign and representing over
distended fetal stomach and proximal duodenum.


![DERIVATIVES OF FOREGUT
• Trachea and respiratory tract
• Lungs
• Esophagus
• Stomach
• Liver gall bladder and bile ducts
• Pancreas (dorsal and ventral)
• Upper duodenum
• Mesentery [dorsal and ventral mesogastrium]](https://image.slidesharecdn.com/developmentofgit3-251120164643-5bd19c2a/85/DEVELOPMENT_OF_GIT_-pptx-11-320.jpg)
![ESOPHAGUS AND TRACHEA:-The region of foregut just
caudal to the pharynx develops two longitudinal ridges
called the tracheoesophageal folds that divide the tube
ventrally into trachea (and subsequent lung buds), and
dorsally into the esophagus.
STOMACH :- It appears as a fusiform dilation of the foregut
endoderm which undergoes a 90 rotation such that the left
◦
side moves ventrally and the right moves dorsally [the vagus
nerve follows this rotation which is how the left vagus
becomes anterior and the right vagus becomes posterior].](https://image.slidesharecdn.com/developmentofgit3-251120164643-5bd19c2a/85/DEVELOPMENT_OF_GIT_-pptx-12-320.jpg)
![DERIVATIVES OF MIDGUT
• Lower duodenum
• Jejunum
• Ileum
• Caecum
• Appendix
• Ascending colon
• Proximal transverse 2/3rd
colon
• Mesentery [small bowel mesentery, mesoappendix ,
transverse mesocolon]](https://image.slidesharecdn.com/developmentofgit3-251120164643-5bd19c2a/85/DEVELOPMENT_OF_GIT_-pptx-20-320.jpg)
![DISTAL DUODENUM:- Distal or lower duodenum arises
from the cranial most portion of the midgut and is served
by anterior and posterior branches of the inferior
pancreaticoduodenal artery, branch of SMA.
JEJUNUM, ILEUM PORTION OF LARGE INTESTINE FROM
MIDGUT:- Midgut elongates rapidly beyond the capacity of
the embryonic abdominal cavity and thus forms a u shaped
loop that herniates into the umbilicus and is oriented
parallel to axis of the embryo such that there is an upper or
cranial loop[jejunum and upper pat of ileum] and a lower or
caudal loop.](https://image.slidesharecdn.com/developmentofgit3-251120164643-5bd19c2a/85/DEVELOPMENT_OF_GIT_-pptx-21-320.jpg)


![DERIVATIVES OF HINDGUT
• Distal 1/3rd
transverse colon
• Descending colon
• Sigmoid colon
• Rectum
• Upper anal canal
• Urogenital sinus
• Mesentery [ transverse mesocolon , sigmoid mesocolon]](https://image.slidesharecdn.com/developmentofgit3-251120164643-5bd19c2a/85/DEVELOPMENT_OF_GIT_-pptx-24-320.jpg)
![ANOMALIES OF
MIDGUT
1]OMPHALOCELE
2]GASTROSCHISIS
3]MECKEL DIVERTICULUM
4]MALROTATION
5]DUODENAL ATRESIA/STENOSIS](https://image.slidesharecdn.com/developmentofgit3-251120164643-5bd19c2a/85/DEVELOPMENT_OF_GIT_-pptx-29-320.jpg)
![1]OMPHALOCELE
• A/K/A EXOMPHALOS , are congenital midline abdominal
wall defects at the base of the umbilical cord insertion, with
herniation of gut [or occasionally other structures ] out of
the fetal abdomen.
• USG:- multiple bowel loops (and on occasion liver) herniate
into a membrane-covered defect (i.e. not free-flowing) and
are usually seen as hyperechogenic content (non-fluid filled
bowel)
• the umbilical cord insertion is directly into the omphalocele](https://image.slidesharecdn.com/developmentofgit3-251120164643-5bd19c2a/85/DEVELOPMENT_OF_GIT_-pptx-30-320.jpg)
![2]GASTROSCHISIS
• Extra-abdominal herniation of fetal or neonatal bowel loops (and
occasionally portions of the stomach , liver , and/or gall bladder)
into the amniotic cavity through a para-umbilical anterior
abdominal wall defect.
• USG:-The herniated content is towards the right side of the
umbilical cord in most cases; color Doppler may be useful to locate
the cord in relation to the herniation. This causes the fetal
abdominal circumference to be smaller than expected for
gestation age. The herniated bowel often appears free-floating
rather than contained. The herniated bowel wall can be thickened
due to edema.
• There can be either accompanying oligohydramnios or
polyhydramnios as ancillary sonographic sonographic features.](https://image.slidesharecdn.com/developmentofgit3-251120164643-5bd19c2a/85/DEVELOPMENT_OF_GIT_-pptx-34-320.jpg)


![3]MECKEL DIVERTICULUM
• Remnant of the vitelline duct, which connects the yolk sac to the
midgut through the umbilical cord. This duct is typically
obliterated by the 5th
to 8th
week of gestation.
• Fluoroscopy
• Small bowel enemas have sometimes been used for the diagnosis
in some centers, although a precise technique is required if the
diagnosis is to be excluded with any degree of certainty 4
.
• Ultrasound
• Usually of limited use in the diagnosis of an uncomplicated
Meckel diverticulum. Ultrasound may show a blind-ending
peristaltic loop connected to the small bowel - it may have a
multi-layered appearance of the wall.](https://image.slidesharecdn.com/developmentofgit3-251120164643-5bd19c2a/85/DEVELOPMENT_OF_GIT_-pptx-37-320.jpg)
![4]MALROTATION
• In the developing embryo growth of the bowel requires herniation
into the omphalomesenteric sac.
In the tenth week of gestation the bowel returns to the abdominal
cavity.
• This return is accompanied by a counterclockwise rotation of the
midgut to achieve its final position with the ligament of Treitz in the
left upper quadrant and the caecum in the right lower quadrant,
suspended from a long mesentery.
• Malrotation arises when the rotation is arrested or even reversed.
As a result the bowel has an abnormal position, the mesentery is
short and peritoneal bands, called Ladd's bands, may cross from the
caecum to the liver or to the anterior abdominal wall.](https://image.slidesharecdn.com/developmentofgit3-251120164643-5bd19c2a/85/DEVELOPMENT_OF_GIT_-pptx-40-320.jpg)

![5] DUODENAL ATRESIA/STENOSIS
• Duodenal atresia results from a congenital malformation of
the duodenum and requires prompt correction in the
neonatal period. It is considered to be one of the
commonest causes of fetal bowel obstruction.
• Plain radiograph
• Abdominal radiographs may classically show a
double bubble sign with gas filled distended stomach and
duodenum with an absence of distal gas. A similar
appearance (either filled with fluid or gas) can be seen in
other modalities.](https://image.slidesharecdn.com/developmentofgit3-251120164643-5bd19c2a/85/DEVELOPMENT_OF_GIT_-pptx-51-320.jpg)









































![imaging_in_lung_cancer[1] - Read-Only.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/imaginginlungcancer1-read-only-251017162350-e8ae4014-thumbnail.jpg?width=640&height=640&fit=bounds)






![OESOPHAGEAL ANATOMY AND PATHOLOGIES (2) [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/oesophagealanatomyandpathologies2autosaved-250917094352-40c57836-thumbnail.jpg?width=640&height=640&fit=bounds)




















