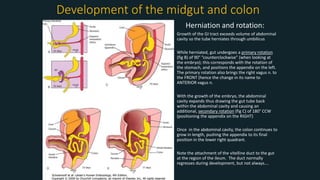
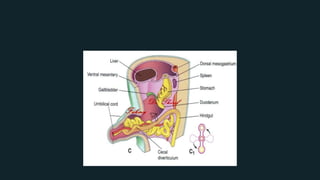
1. The midgut forms a U-shaped loop that herniates through the umbilical ring and undergoes two rotations to return to the abdominal cavity, positioning the appendix on the right.
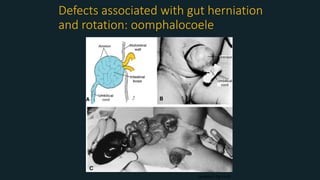
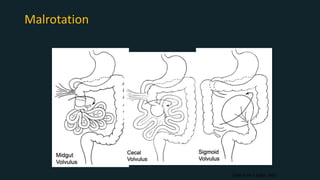
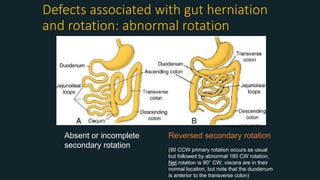
2. Failure of the midgut to return or complete rotation can result in defects like omphalocele, malrotation, intestinal atresia or stenosis.
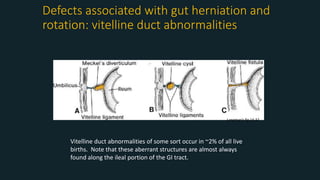
3. Common midgut defects include Meckel's diverticulum from persistence of the vitelline duct and intestinal malrotation from incomplete rotation.