Downloaded 122 times


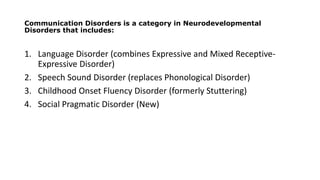
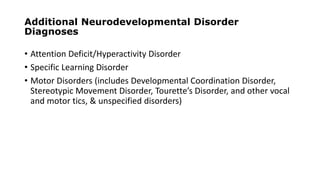
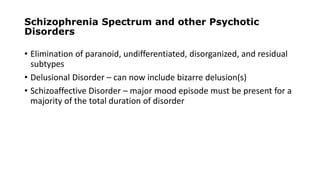
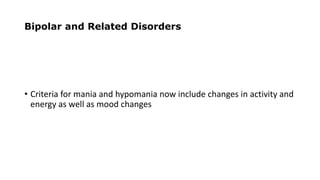
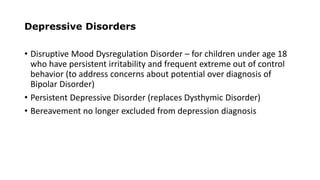
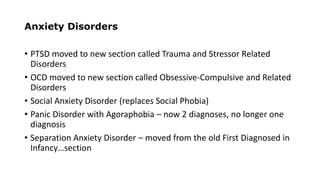
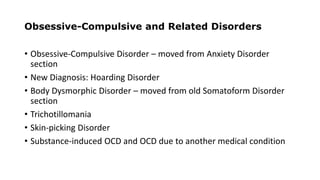
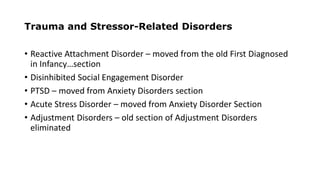


The document provides an overview of the history and development of the Diagnostic and Statistical Manual of Mental Disorders (DSM). It discusses the key changes between editions, from the initial DSM-I in 1952 to the current DSM-5 from 2013. Major revisions in DSM-5 include eliminating the multi-axial system, replacing many disorder names, combining and reorganizing certain diagnoses, and emphasizing dimensional assessments and cultural factors in diagnosis. The goal is to improve clinical utility, reliability and cultural sensitivity in defining and classifying mental disorders.























































































