Downloaded 47 times


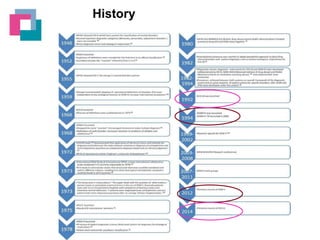
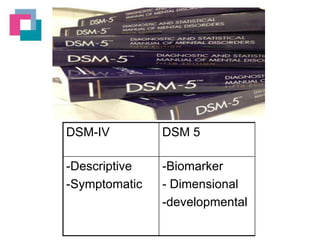
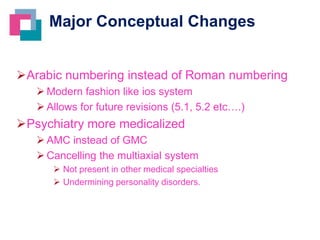
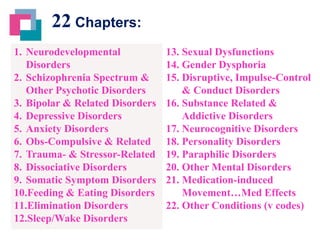





The document summarizes some of the major changes between the DSM-IV and the newly released DSM-5. Some key points: 1) The DSM-5 removes the multiaxial system of diagnosis and replaces it with a new assessment approach without arbitrary boundaries between disorders. 2) Several new disorders have been added, some combined, and a few eliminated. The number of chapters has increased from 17 to 22. 3) Each diagnosis now follows a standardized structure providing diagnostic criteria, prevalence, course, and differential diagnosis. 4) Future revisions will use a "living document" approach denoted by numbers (e.g. DSM-5.1) instead of Roman numer

































































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)









