Downloaded 36 times
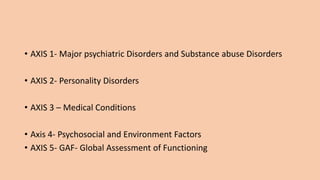
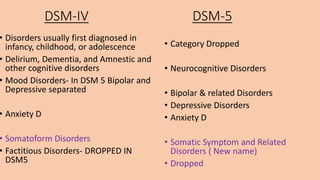

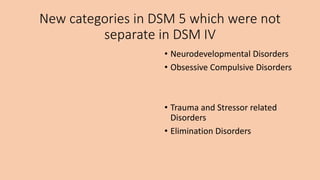
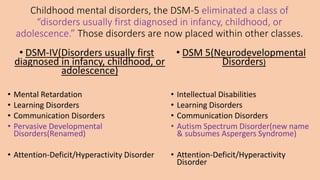
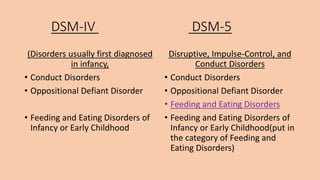

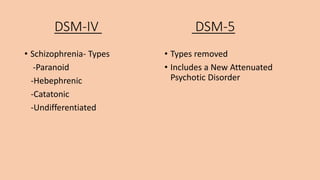
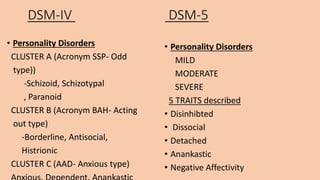
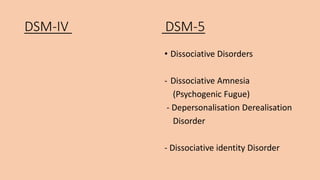
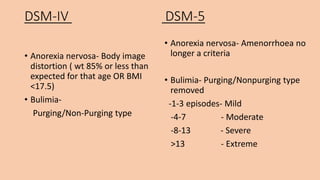


The document summarizes some of the key differences between the DSM-IV and DSM-5 diagnostic manuals. Some of the main changes include: - The DSM-5 removed the multiaxial system that was used in DSM-IV. - Several disorders were renamed or reclassified, such as moving obsessive-compulsive disorder into its own category. - New disorders were added, like disruptive mood dysregulation disorder in children. - Criteria for some existing disorders were updated, like changing the definitions for bipolar disorders and anorexia nervosa. - The number of diagnoses grew from 365 in the DSM-IV to over 500 in the DSM

























![Psychodiagnostic technique[1]](https://cdn.slidesharecdn.com/ss_thumbnails/psychodiagnostictechnique1-191031121907-thumbnail.jpg?width=640&height=640&fit=bounds)









































