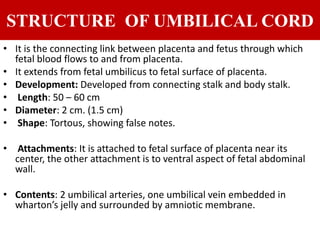
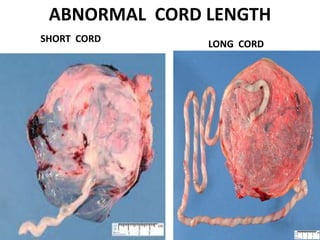
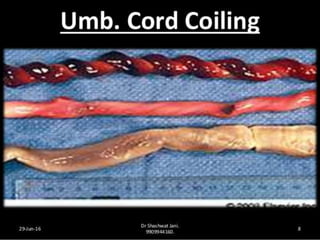

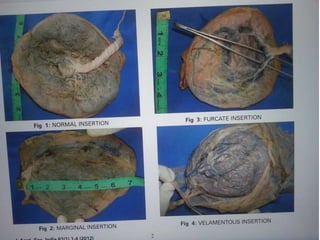
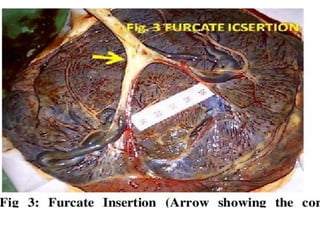

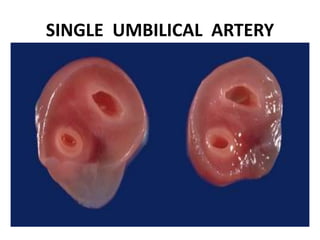
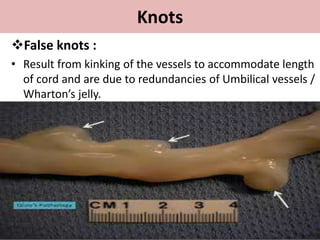
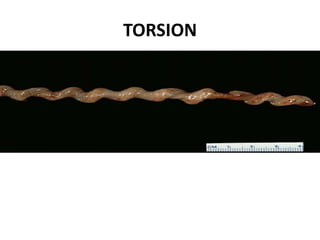
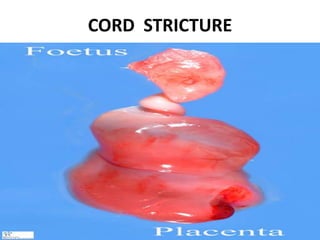

The document discusses the structure and abnormalities of the umbilical cord. It notes that the cord normally measures 50-60 cm in length and contains two umbilical arteries and one vein embedded in Wharton's jelly. Abnormalities include short or long cord length, abnormal diameter, single umbilical artery, knots, cysts, and abnormal cord insertion or coiling. Certain abnormalities like short cords or single umbilical artery can increase risks of fetal distress, preterm delivery, or growth restriction.























































































