Downloaded 1,230 times

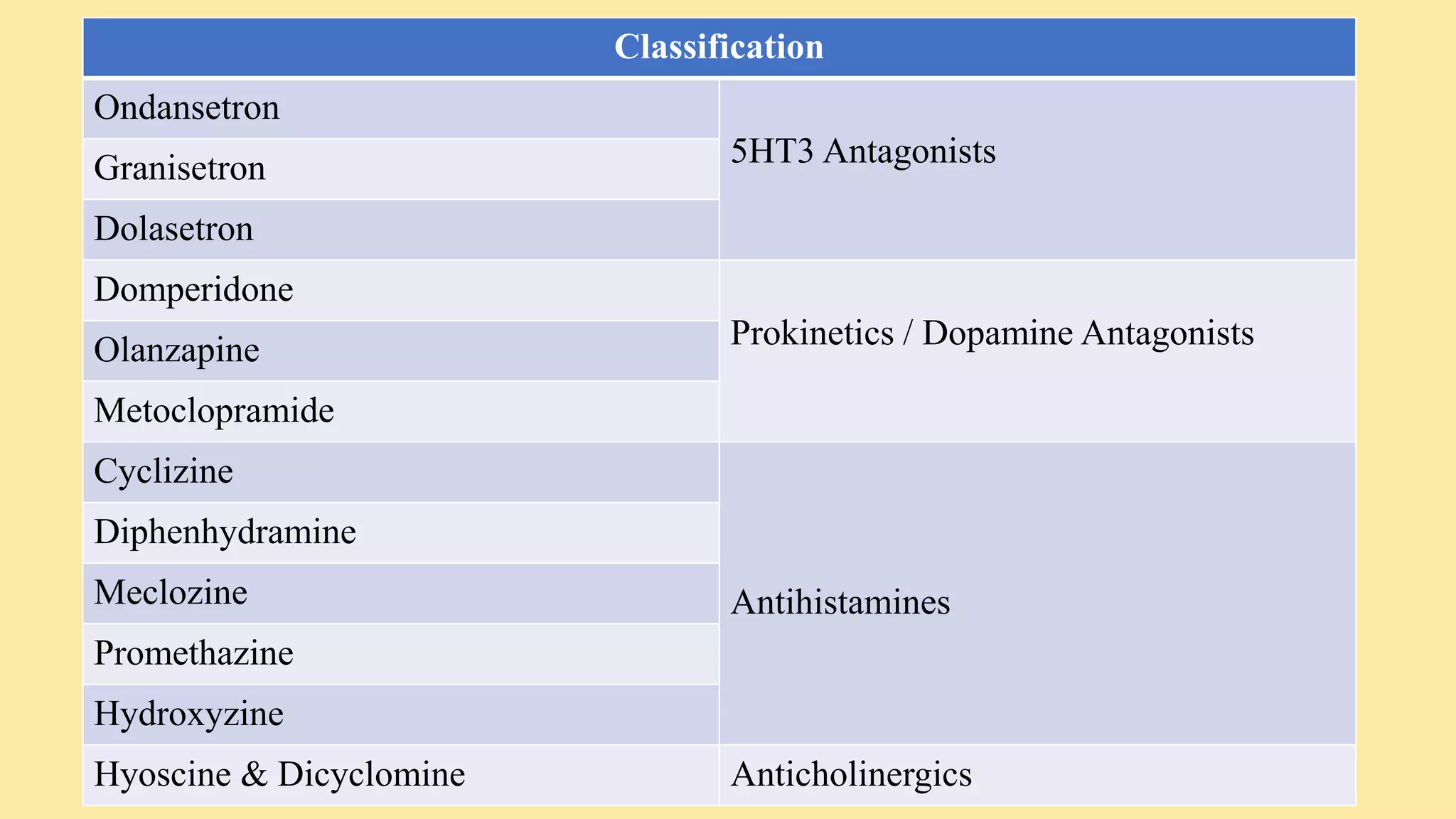
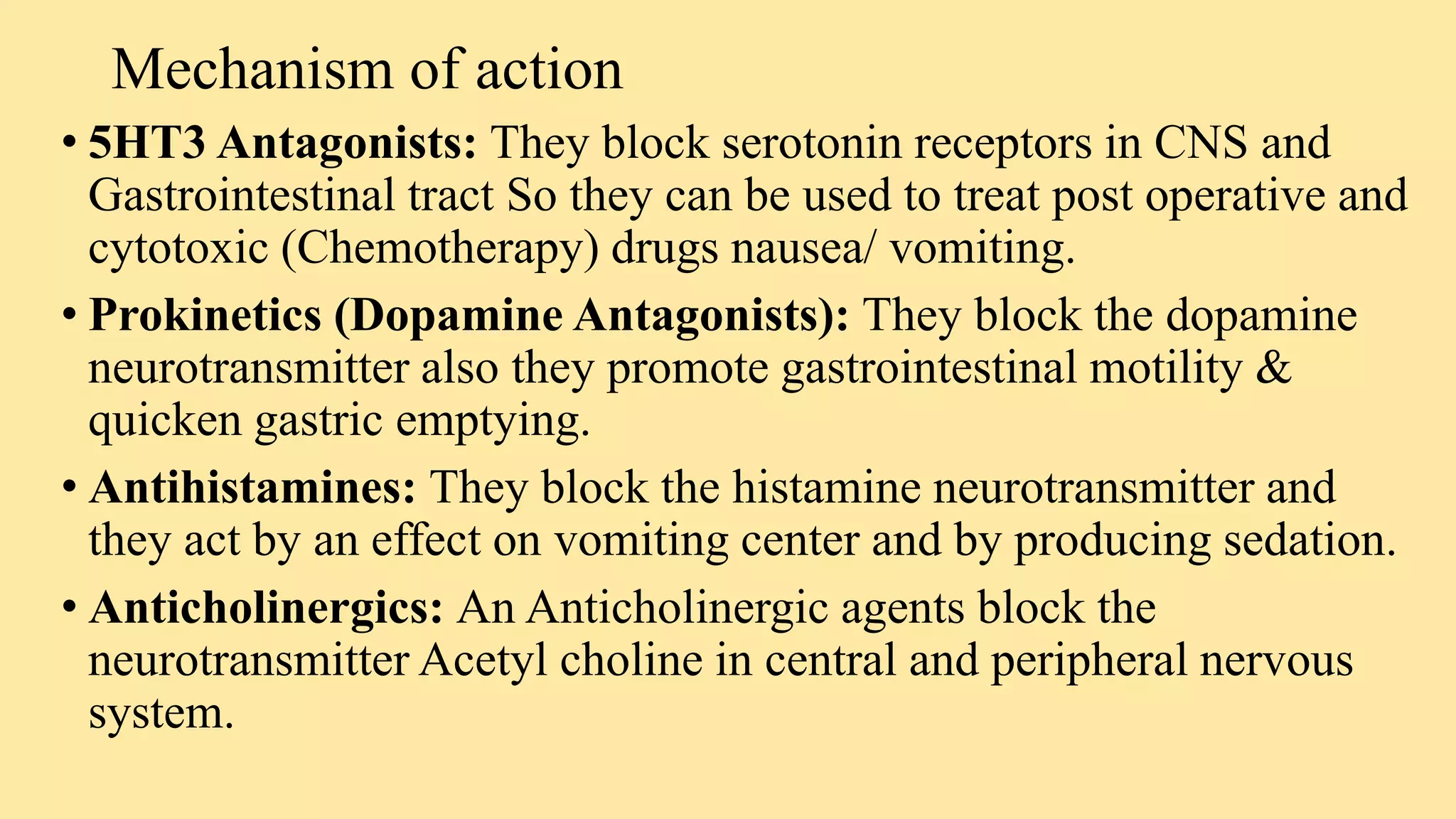
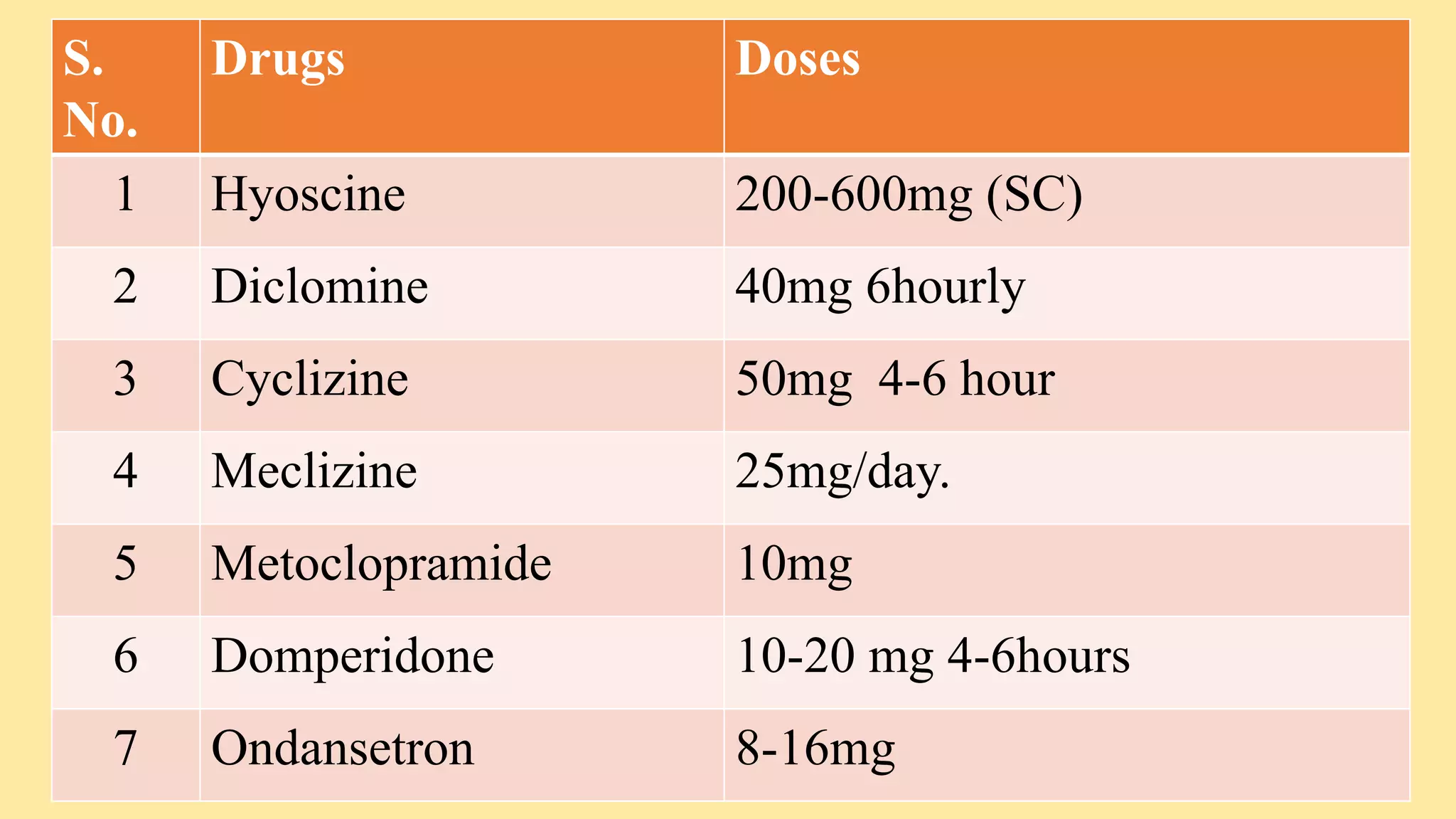









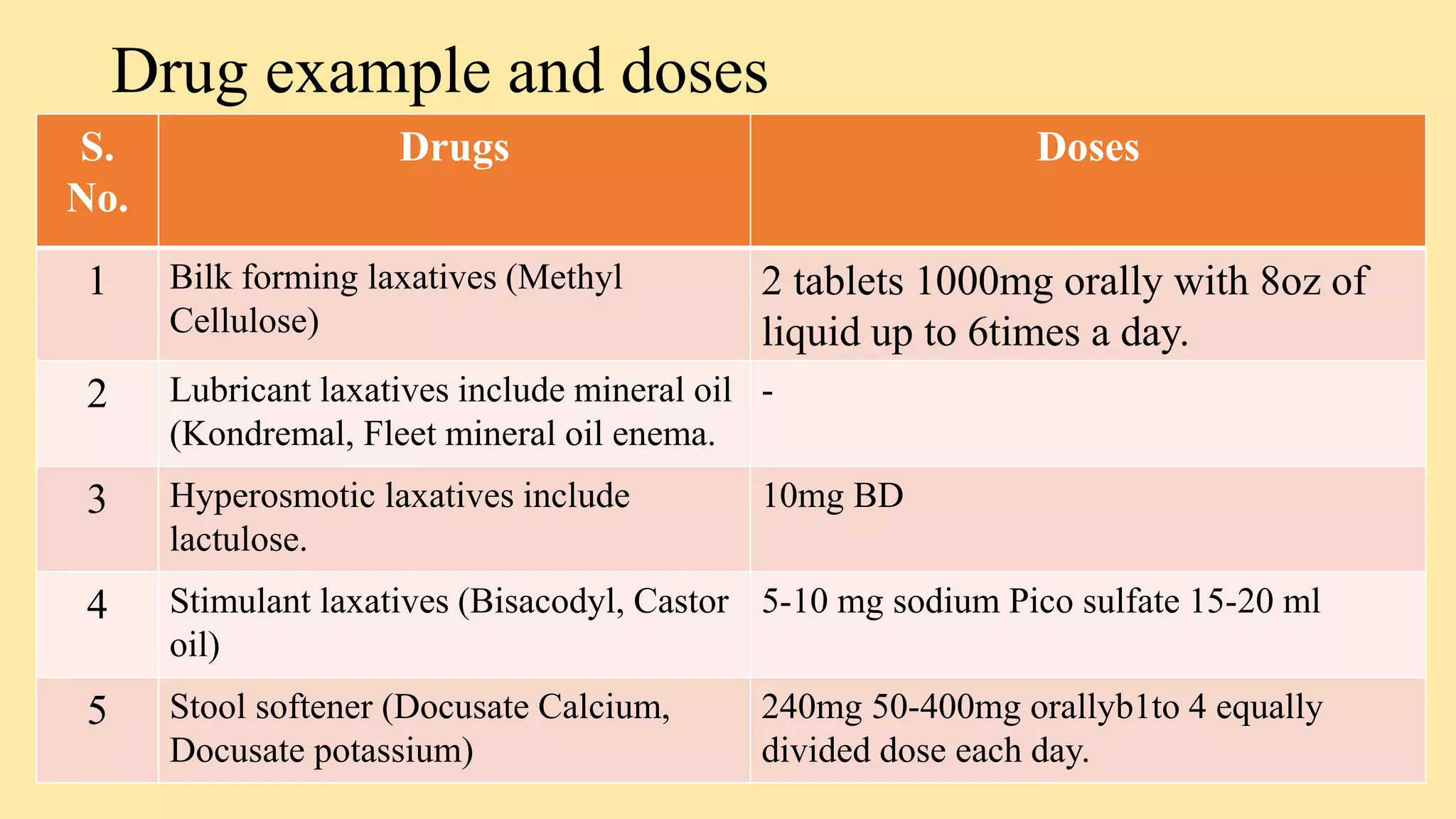



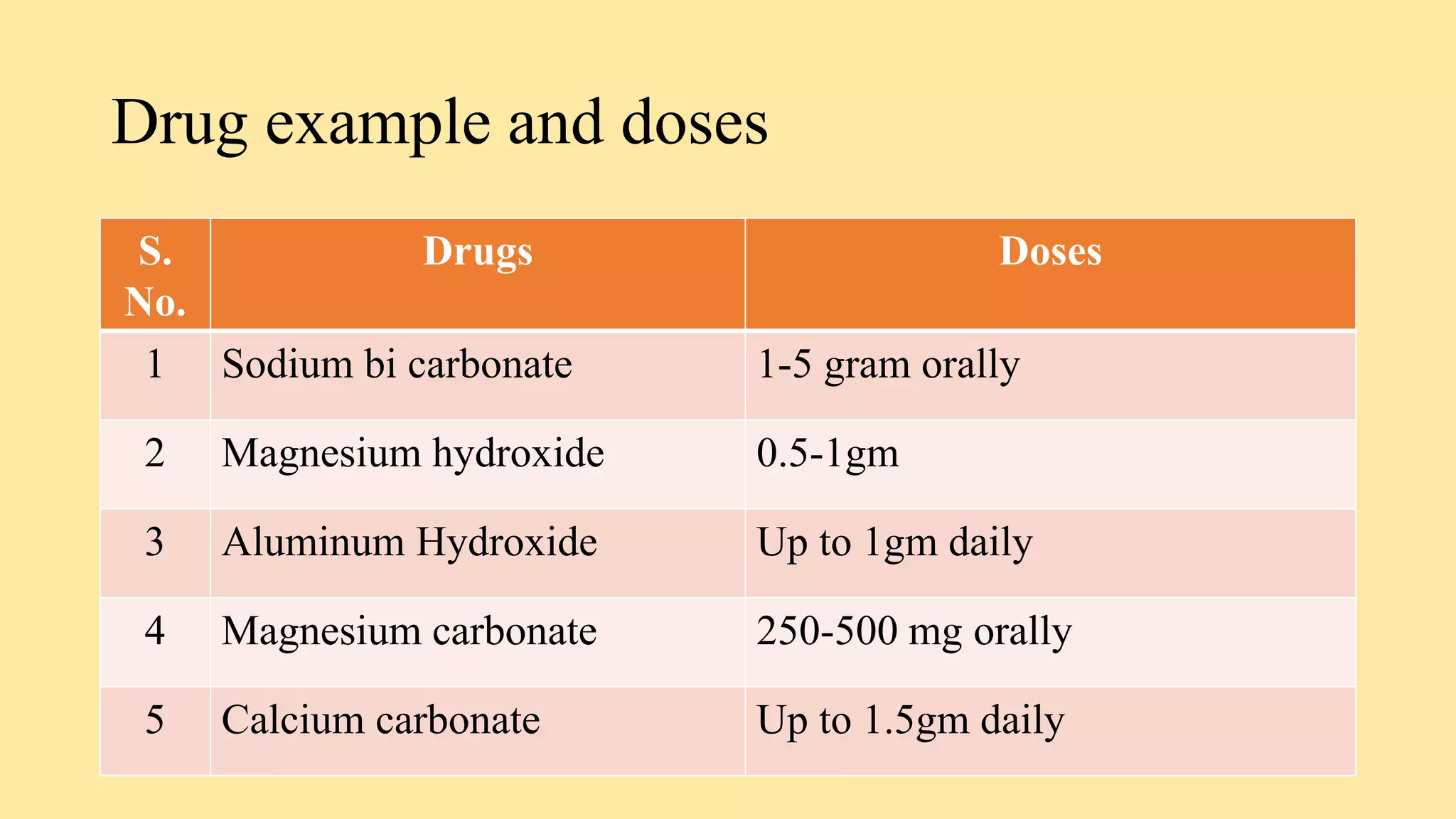




























Drugs acting on the GI system include: - Antiemetics which prevent nausea and vomiting like ondansetron and metoclopramide. - Laxatives and purgatives like lactulose, bisacodyl, and docusate which are used to treat constipation. - Antacids such as aluminum hydroxide, magnesium hydroxide, and calcium carbonate which neutralize stomach acid. - Cholinergic drugs which increase GI motility and secretions. Anticholinergic drugs block acetylcholine and decrease motility and secretions.




















































































