Downloaded 2,798 times
















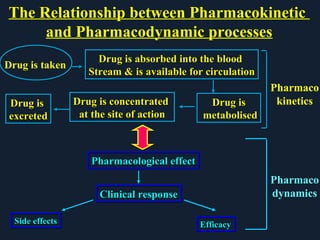





The document provides an introduction to pharmacology, covering its definitions, history, types, and classification of drugs. It explores the actions, therapeutic uses, adverse effects, and interactions of drugs, emphasizing the importance of rational drug use and the role of pharmacologists. Additionally, it discusses various drug sources, terminology, and the evolution of pharmacology as a scientific discipline.



















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)