Threatened abortion by dr alka mukherjee dr apurva mukherjee nagpur m.s.alka mukherjee
Threatened abortion is associated with bleeding and/or uterine cramping while the cervix is closed. This stage of abortion may progress to spontaneous incomplete or complete abortion. While this event may be considered a part of the quality control process in human reproduction, it is important to know the possible etiologies and when therapy might prevent pregnancy loss. The World Health Organization estimated that 15% of all clinically recognizable pregnancies and in spontaneous abortion, 50-60% of which are due to chromosomal abnormalities. Apart from the fetal factors, several maternal and probably paternal factors contribute to the causes of spontaneous abortion. The maternal factors that may be responsible for abortion include both local and systemic conditions such as infections, maternal disease states, genital tract abnormalities, endocrine factors and other miscellaneous causes (antiphospholipid antibodies, maternal-fetal histocompatibility, excessive smoking and other environmental toxicants, etc.). This review focuses on the management of threatened abortion, but it should be emphasized that the management to maintain pregnancy is reasonable only in those cases, in which the fetus is not seriously affected. It would not be beneficial to provide treatment that would permit chromosomally and anatomically abnormal embryos to survive to term. Treatment is feasible first of all in cases with maternal factors. Surgical procedures may precede pregnancy (correction of septate uterus, removal of a submucous leiomyomata) or may be performed usually in the second trimester (cervical cerclage). Maternal general diseases (diabetes, hypothyroidism) and infections should be treated accordingly. The most common entity to be treated in this category is luteal phase deficiency. Progesterone is the most important hormone for the maintenance of an early human pregnancy. Besides progesterone administration, human chorionic gonadotropin (hCG) also is the logical endocrine treatment of choice. In the pregnant woman hCG stimulates and optimizes hormonal production in the corpus luteum and may also influence the fetoplacental unit. The contribution of environmental, physical and chemical agents to the incidence of spontaneous abortion is controversial. They may be abortifacient even if they are not teratogenic. Exposure to environmental toxicants should be avoided. Paternal leukocyte immunotherapy has been associated with successful outcome in patients with unexplained repeated spontaneous abortion. This therapeutic approach is considered experimental, as there may be some significant risks. Associating maternal antiphospholipid antibodies with reproductive failure is a rapidly developing field. Administration of corticosteroids with low doses of aspirin has resulted in fetal salvage in women in whom antiphospholipid antibodies are present.
Threatened abortion by dr alka mukherjee dr apurva mukherjee nagpur m.s.alka mukherjee
Threatened abortion is associated with bleeding and/or uterine cramping while the cervix is closed. This stage of abortion may progress to spontaneous incomplete or complete abortion. While this event may be considered a part of the quality control process in human reproduction, it is important to know the possible etiologies and when therapy might prevent pregnancy loss. The World Health Organization estimated that 15% of all clinically recognizable pregnancies and in spontaneous abortion, 50-60% of which are due to chromosomal abnormalities. Apart from the fetal factors, several maternal and probably paternal factors contribute to the causes of spontaneous abortion. The maternal factors that may be responsible for abortion include both local and systemic conditions such as infections, maternal disease states, genital tract abnormalities, endocrine factors and other miscellaneous causes (antiphospholipid antibodies, maternal-fetal histocompatibility, excessive smoking and other environmental toxicants, etc.). This review focuses on the management of threatened abortion, but it should be emphasized that the management to maintain pregnancy is reasonable only in those cases, in which the fetus is not seriously affected. It would not be beneficial to provide treatment that would permit chromosomally and anatomically abnormal embryos to survive to term. Treatment is feasible first of all in cases with maternal factors. Surgical procedures may precede pregnancy (correction of septate uterus, removal of a submucous leiomyomata) or may be performed usually in the second trimester (cervical cerclage). Maternal general diseases (diabetes, hypothyroidism) and infections should be treated accordingly. The most common entity to be treated in this category is luteal phase deficiency. Progesterone is the most important hormone for the maintenance of an early human pregnancy. Besides progesterone administration, human chorionic gonadotropin (hCG) also is the logical endocrine treatment of choice. In the pregnant woman hCG stimulates and optimizes hormonal production in the corpus luteum and may also influence the fetoplacental unit. The contribution of environmental, physical and chemical agents to the incidence of spontaneous abortion is controversial. They may be abortifacient even if they are not teratogenic. Exposure to environmental toxicants should be avoided. Paternal leukocyte immunotherapy has been associated with successful outcome in patients with unexplained repeated spontaneous abortion. This therapeutic approach is considered experimental, as there may be some significant risks. Associating maternal antiphospholipid antibodies with reproductive failure is a rapidly developing field. Administration of corticosteroids with low doses of aspirin has resulted in fetal salvage in women in whom antiphospholipid antibodies are present.
Hydatidiform Mole (HM) is a rare mass or growth that forms inside the uterus at the beginning of a pregnancy. It is a type of gestational trophoblastic disease (GTD).
When a normal sperm cell fertilizes one of these oocytes, the resulting embryo has only one set of chromosomes. Because the embryo has no genes from the mother, the pregnancy cannot develop normally, resulting in a hydatidiform mole.
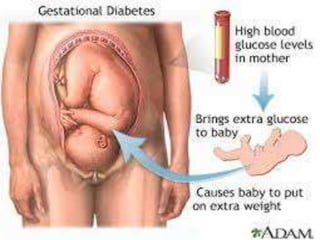
- gestational DM is critical metabolic disorder during pregnancy .
- According to a 2014 analysis by the Centers for Disease Control and Prevention, the prevalence of gestational diabetes is as high as 9.2%
- this presentation is about Gestational DM , introduction , diagnostic criteria , principles of approach and treatment and the sequels of such pregnancy and it`s effect of coming infant .
- this presentation is done by ; Dr. Nawras Mahir Farhan .
- References : most info.s in this presentation , from Dewhurst's Textbook of Obstetrics and Gynaecology, gynecology and obstetrics by ten teachers .
Hydatidiform Mole (HM) is a rare mass or growth that forms inside the uterus at the beginning of a pregnancy. It is a type of gestational trophoblastic disease (GTD).
When a normal sperm cell fertilizes one of these oocytes, the resulting embryo has only one set of chromosomes. Because the embryo has no genes from the mother, the pregnancy cannot develop normally, resulting in a hydatidiform mole.
- gestational DM is critical metabolic disorder during pregnancy .
- According to a 2014 analysis by the Centers for Disease Control and Prevention, the prevalence of gestational diabetes is as high as 9.2%
- this presentation is about Gestational DM , introduction , diagnostic criteria , principles of approach and treatment and the sequels of such pregnancy and it`s effect of coming infant .
- this presentation is done by ; Dr. Nawras Mahir Farhan .
- References : most info.s in this presentation , from Dewhurst's Textbook of Obstetrics and Gynaecology, gynecology and obstetrics by ten teachers .
The Primary Care Physician's guide to management of Pregnancy DiabetesHanifullah Khan
A guide on the screening, diagnosis and management of diabetes in pregnancy aimed at facilitating the handling of this condition in a primary care setting. Includes details on medications and dosages
A comprehensive guide to the management of hyperglycaemia in pregnancy aimed at the primary care physician and based on latest evidenced based criteria. Includes information from latest studies such as HAPO study and ACHOIS, and involves guidelines from the IADPSG, ADA, WHO and Malaysia.
263778731218 Abortion Clinic /Pills In Harare ,sisternakatoto
263778731218 Abortion Clinic /Pills In Harare ,ABORTION WOMEN’S CLINIC +27730423979 IN women clinic we believe that every woman should be able to make choices in her pregnancy. Our job is to provide compassionate care, safety,affordable and confidential services. That’s why we have won the trust from all generations of women all over the world. we use non surgical method(Abortion pills) to terminate…Dr.LISA +27730423979women Clinic is committed to providing the highest quality of obstetrical and gynecological care to women of all ages. Our dedicated staff aim to treat each patient and her health concerns with compassion and respect.Our dedicated group ABORTION WOMEN’S CLINIC +27730423979 IN women clinic we believe that every woman should be able to make choices in her pregnancy. Our job is to provide compassionate care, safety,affordable and confidential services. That’s why we have won the trust from all generations of women all over the world. we use non surgical method(Abortion pills) to terminate…Dr.LISA +27730423979women Clinic is committed to providing the highest quality of obstetrical and gynecological care to women of all ages. Our dedicated staff aim to treat each patient and her health concerns with compassion and respect.Our dedicated group of receptionists, nurses, and physicians have worked together as a teamof receptionists, nurses, and physicians have worked together as a team wwww.lisywomensclinic.co.za/
micro teaching on communication m.sc nursing.pdfAnurag Sharma
Microteaching is a unique model of practice teaching. It is a viable instrument for the. desired change in the teaching behavior or the behavior potential which, in specified types of real. classroom situations, tends to facilitate the achievement of specified types of objectives.
New Drug Discovery and Development .....NEHA GUPTA
The "New Drug Discovery and Development" process involves the identification, design, testing, and manufacturing of novel pharmaceutical compounds with the aim of introducing new and improved treatments for various medical conditions. This comprehensive endeavor encompasses various stages, including target identification, preclinical studies, clinical trials, regulatory approval, and post-market surveillance. It involves multidisciplinary collaboration among scientists, researchers, clinicians, regulatory experts, and pharmaceutical companies to bring innovative therapies to market and address unmet medical needs.
Ozempic: Preoperative Management of Patients on GLP-1 Receptor Agonists Saeid Safari
Preoperative Management of Patients on GLP-1 Receptor Agonists like Ozempic and Semiglutide
ASA GUIDELINE
NYSORA Guideline
2 Case Reports of Gastric Ultrasound
Recomendações da OMS sobre cuidados maternos e neonatais para uma experiência pós-natal positiva.
Em consonância com os ODS – Objetivos do Desenvolvimento Sustentável e a Estratégia Global para a Saúde das Mulheres, Crianças e Adolescentes, e aplicando uma abordagem baseada nos direitos humanos, os esforços de cuidados pós-natais devem expandir-se para além da cobertura e da simples sobrevivência, de modo a incluir cuidados de qualidade.
Estas diretrizes visam melhorar a qualidade dos cuidados pós-natais essenciais e de rotina prestados às mulheres e aos recém-nascidos, com o objetivo final de melhorar a saúde e o bem-estar materno e neonatal.
Uma “experiência pós-natal positiva” é um resultado importante para todas as mulheres que dão à luz e para os seus recém-nascidos, estabelecendo as bases para a melhoria da saúde e do bem-estar a curto e longo prazo. Uma experiência pós-natal positiva é definida como aquela em que as mulheres, pessoas que gestam, os recém-nascidos, os casais, os pais, os cuidadores e as famílias recebem informação consistente, garantia e apoio de profissionais de saúde motivados; e onde um sistema de saúde flexível e com recursos reconheça as necessidades das mulheres e dos bebês e respeite o seu contexto cultural.
Estas diretrizes consolidadas apresentam algumas recomendações novas e já bem fundamentadas sobre cuidados pós-natais de rotina para mulheres e neonatos que recebem cuidados no pós-parto em unidades de saúde ou na comunidade, independentemente dos recursos disponíveis.
É fornecido um conjunto abrangente de recomendações para cuidados durante o período puerperal, com ênfase nos cuidados essenciais que todas as mulheres e recém-nascidos devem receber, e com a devida atenção à qualidade dos cuidados; isto é, a entrega e a experiência do cuidado recebido. Estas diretrizes atualizam e ampliam as recomendações da OMS de 2014 sobre cuidados pós-natais da mãe e do recém-nascido e complementam as atuais diretrizes da OMS sobre a gestão de complicações pós-natais.
O estabelecimento da amamentação e o manejo das principais intercorrências é contemplada.
Recomendamos muito.
Vamos discutir essas recomendações no nosso curso de pós-graduação em Aleitamento no Instituto Ciclos.
Esta publicação só está disponível em inglês até o momento.
Prof. Marcus Renato de Carvalho
www.agostodourado.com
Title: Sense of Smell
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the primary categories of smells and the concept of odor blindness.
Explain the structure and location of the olfactory membrane and mucosa, including the types and roles of cells involved in olfaction.
Describe the pathway and mechanisms of olfactory signal transmission from the olfactory receptors to the brain.
Illustrate the biochemical cascade triggered by odorant binding to olfactory receptors, including the role of G-proteins and second messengers in generating an action potential.
Identify different types of olfactory disorders such as anosmia, hyposmia, hyperosmia, and dysosmia, including their potential causes.
Key Topics:
Olfactory Genes:
3% of the human genome accounts for olfactory genes.
400 genes for odorant receptors.
Olfactory Membrane:
Located in the superior part of the nasal cavity.
Medially: Folds downward along the superior septum.
Laterally: Folds over the superior turbinate and upper surface of the middle turbinate.
Total surface area: 5-10 square centimeters.
Olfactory Mucosa:
Olfactory Cells: Bipolar nerve cells derived from the CNS (100 million), with 4-25 olfactory cilia per cell.
Sustentacular Cells: Produce mucus and maintain ionic and molecular environment.
Basal Cells: Replace worn-out olfactory cells with an average lifespan of 1-2 months.
Bowman’s Gland: Secretes mucus.
Stimulation of Olfactory Cells:
Odorant dissolves in mucus and attaches to receptors on olfactory cilia.
Involves a cascade effect through G-proteins and second messengers, leading to depolarization and action potential generation in the olfactory nerve.
Quality of a Good Odorant:
Small (3-20 Carbon atoms), volatile, water-soluble, and lipid-soluble.
Facilitated by odorant-binding proteins in mucus.
Membrane Potential and Action Potential:
Resting membrane potential: -55mV.
Action potential frequency in the olfactory nerve increases with odorant strength.
Adaptation Towards the Sense of Smell:
Rapid adaptation within the first second, with further slow adaptation.
Psychological adaptation greater than receptor adaptation, involving feedback inhibition from the central nervous system.
Primary Sensations of Smell:
Camphoraceous, Musky, Floral, Pepperminty, Ethereal, Pungent, Putrid.
Odor Detection Threshold:
Examples: Hydrogen sulfide (0.0005 ppm), Methyl-mercaptan (0.002 ppm).
Some toxic substances are odorless at lethal concentrations.
Characteristics of Smell:
Odor blindness for single substances due to lack of appropriate receptor protein.
Behavioral and emotional influences of smell.
Transmission of Olfactory Signals:
From olfactory cells to glomeruli in the olfactory bulb, involving lateral inhibition.
Primitive, less old, and new olfactory systems with different path
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Ve...kevinkariuki227
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Verified Chapters 1 - 19, Complete Newest Version.pdf
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Verified Chapters 1 - 19, Complete Newest Version.pdf
Explore natural remedies for syphilis treatment in Singapore. Discover alternative therapies, herbal remedies, and lifestyle changes that may complement conventional treatments. Learn about holistic approaches to managing syphilis symptoms and supporting overall health.
HOT NEW PRODUCT! BIG SALES FAST SHIPPING NOW FROM CHINA!! EU KU DB BK substit...GL Anaacs
Contact us if you are interested:
Email / Skype : kefaya1771@gmail.com
Threema: PXHY5PDH
New BATCH Ku !!! MUCH IN DEMAND FAST SALE EVERY BATCH HAPPY GOOD EFFECT BIG BATCH !
Contact me on Threema or skype to start big business!!
Hot-sale products:
NEW HOT EUTYLONE WHITE CRYSTAL!!
5cl-adba precursor (semi finished )
5cl-adba raw materials
ADBB precursor (semi finished )
ADBB raw materials
APVP powder
5fadb/4f-adb
Jwh018 / Jwh210
Eutylone crystal
Protonitazene (hydrochloride) CAS: 119276-01-6
Flubrotizolam CAS: 57801-95-3
Metonitazene CAS: 14680-51-4
Payment terms: Western Union,MoneyGram,Bitcoin or USDT.
Deliver Time: Usually 7-15days
Shipping method: FedEx, TNT, DHL,UPS etc.Our deliveries are 100% safe, fast, reliable and discreet.
Samples will be sent for your evaluation!If you are interested in, please contact me, let's talk details.
We specializes in exporting high quality Research chemical, medical intermediate, Pharmaceutical chemicals and so on. Products are exported to USA, Canada, France, Korea, Japan,Russia, Southeast Asia and other countries.
Ethanol (CH3CH2OH), or beverage alcohol, is a two-carbon alcohol
that is rapidly distributed in the body and brain. Ethanol alters many
neurochemical systems and has rewarding and addictive properties. It
is the oldest recreational drug and likely contributes to more morbidity,
mortality, and public health costs than all illicit drugs combined. The
5th edition of the Diagnostic and Statistical Manual of Mental Disorders
(DSM-5) integrates alcohol abuse and alcohol dependence into a single
disorder called alcohol use disorder (AUD), with mild, moderate,
and severe subclassifications (American Psychiatric Association, 2013).
In the DSM-5, all types of substance abuse and dependence have been
combined into a single substance use disorder (SUD) on a continuum
from mild to severe. A diagnosis of AUD requires that at least two of
the 11 DSM-5 behaviors be present within a 12-month period (mild
AUD: 2–3 criteria; moderate AUD: 4–5 criteria; severe AUD: 6–11 criteria).
The four main behavioral effects of AUD are impaired control over
drinking, negative social consequences, risky use, and altered physiological
effects (tolerance, withdrawal). This chapter presents an overview
of the prevalence and harmful consequences of AUD in the U.S.,
the systemic nature of the disease, neurocircuitry and stages of AUD,
comorbidities, fetal alcohol spectrum disorders, genetic risk factors, and
pharmacotherapies for AUD.
Report Back from SGO 2024: What’s the Latest in Cervical Cancer?bkling
Are you curious about what’s new in cervical cancer research or unsure what the findings mean? Join Dr. Emily Ko, a gynecologic oncologist at Penn Medicine, to learn about the latest updates from the Society of Gynecologic Oncology (SGO) 2024 Annual Meeting on Women’s Cancer. Dr. Ko will discuss what the research presented at the conference means for you and answer your questions about the new developments.
The prostate is an exocrine gland of the male mammalian reproductive system
It is a walnut-sized gland that forms part of the male reproductive system and is located in front of the rectum and just below the urinary bladder
Function is to store and secrete a clear, slightly alkaline fluid that constitutes 10-30% of the volume of the seminal fluid that along with the spermatozoa, constitutes semen
A healthy human prostate measures (4cm-vertical, by 3cm-horizontal, 2cm ant-post ).
It surrounds the urethra just below the urinary bladder. It has anterior, median, posterior and two lateral lobes
It’s work is regulated by androgens which are responsible for male sex characteristics
Generalised disease of the prostate due to hormonal derangement which leads to non malignant enlargement of the gland (increase in the number of epithelial cells and stromal tissue)to cause compression of the urethra leading to symptoms (LUTS
3. INTRODUCTION
Diabetes Mellitus is a endocrine and
metabolic disorder in which inability in
carbohydrate ,fat and protien resulting
in raised blood glucose level .
4. Diabetes Mellitus In
Pregnancy
• Diabetes Mellitus is a common medical
disorder encounter in pregnancy.
• Pregnancy is a diabetogenic state due to
insulin resistance increase during
pregnancy .
• Placental hormones are increase during
pregnancy to disturbed insulin action.
5. INCEDENCE
.
•Diabetes remains the 7th leading cause of
death in the united states in 2010.
• According to the National Center for
Heath Statistics [2004] ,iabetes now occurs
in approximately 4 – 14 percent women.
•10 to 20 precent of patient with diabetes
are geststional diabetes.
6. TYPES
Diabetes mellites in pregnancy are 2
types =
1. Pre-gestational Diabetes Mellietes
1. Gestational Diabetes Mellietes
7. 1. Pre-Gestational Diabetes
Mellitus
• In which the diabetes
daigenosed before pregnancy.
• There are mainly 2 types.
1. Type -1 diabetes mellitus
2. Type -2 diabetes mellitus
8. Type-1 Diabetes Mellitus
Also known as the-
•Insulin Dependent Diabetes Mellitus
[IDDM].
•Juvenile Diabetes Mellitus
•It characterized by loss of the insulin
–producing beta cells of the pancreas
leading to insulin deficiency .
9. Pathophysiology and
Risk factors
.
Risk factors =
•Genetic
•Environmental
•Viral infection
Pathophysiology=
•Autoimmune reaction in which the beta
cells that produce insulinare destroyed.
•Alpha cells produce excess glucons
11. Type-2 Diabetes Mellitus
•Also known as Non Insulin Diabetes Mellitus[
NIDDM].
• Type 2 is charactrised by the presens of insulin are
low ,high ,normal and beta cell disfunctioning.
•Type 2 are most common type of diabetes 95 cases.
Risk factors=
•Obesity
•Physical activity
•Family history
•Intacke of high calorie diet
15. DEFINITION
• The word gastation actually refers to
during pregnancy
• Gastational diabetes mellitus is the most
common medical complicatin of
pregnancy
• GDM define as a impaired glucose
tolerence with 1st recognised druring 2&3
trimester(24to28week) of pregnancy
16. RISK FACTORS
Previous history of GDM
positive family history of DM type2
High risk group(aferican
americans,asian american)
Over age > 30 years
Smoking
Obesity
17.
18. HORMONAL CHANGES
PLACENTA
The placenta act as a endocrine organ producing
several important hormones during pregnancy
Placenta produce variety of hormonrs
Steroid
Protien
DURING THE FIRST TRIMESTER
Carpos luteum placenta secreat esteroid hormone
Esteron
progestron
19. •Estrogan and prosteron level are raise in blood
•These hormones estiulates the beta-cell hyperplacia
to secreat insulin
•Promote increase glycogan store
•Decrease hepatic production of glucose
•lead to decrease fasting blood gluse level in the 1st
trimester
20. DURING 2&3 TRIMESTER
*Placenta secreat daibetogenic and protin hormone
Human placental lectose
Estrogen and progestron
Placental insulinase
Increase hepatic glucose production
Decrease hepatic glycogan store
These hormone antagonise insuline effectiveness
Raising placenta hormone increase insulin
registance
Leading to hyperglycemia occuse after meals.
21.
22. PATHOPHYSIOLOGY
• Due to etiological factoes
• During 2&3 trimaster screat placental hormone
(Human placental lectose ,Estrogen and progestron
,Placental insulinase)
these hormone antagonised effect for insulin
increase blood suger level
Body dose not made insulin properly
Matenal blood glucose in fetas throgh placenta
Fetal hyperglycemia
Activated pancreatic hyperplasia of beta-
cell(12week start insulin production)
Insulin increase in fetus
23. EFFECT OF DAIBETES ON PRTEGNANC
• MATENAL EFFECT
• IN PREGNANCY
• Abortion
• Infection
• Prterm labor
• Hypertansion
• Plyhdraminos
• DURING LABOUR
• Sholder distocia
• Prineal injuries
29. INVESTIGATION
• URINE CULTURE
• Should be done at the initial visit at 4-6week
interval to rule out asymptomatic bactoriuria.
• OPTHALMOLOGICAL EXAMINATION
• this is performed in all daibetics at the intial
antenatal examination and develop retinal changes
• RENAL FACTION
• A base line serum cretinine is optain at in the initial
visit and value is more than 0.8 mg/dl .
• Renal fuction is assesd every 4week
• ECG : suspected ischemic heart disease patient
30. MATERNAL SERUM ALFA FECTOPROTIEN:
Estimation is done between 16&20 weeks to screen
the nural tube defect
ULTRASOUND :it is indicate in the 1st trimester for
acurate dating of pregnancy
In eary growth lag ina pregatationa daibetes is an
indicate of a fetal malformation and early abortion
2nd trimester : detail anomalies sacle is perform abt
18-20 weeks
Fetal ecocardiography to rule out cardic anomalies is
done aroud 20-24weeks.
3red trimester: monitor macrosomia .
33. (2)EXERCISE
•Exercise is an important component in maitaining
glucose control
•Improves physical and psycological weelbeing of the
patient
Exercise must be avoided at the peak time of insulin
action.
Exercise sach as
Deepbrithing
Walking
yoga
34. (3)PHARMACOLOGICAL
INSULIN INFUTION:
If a contineously inslin infution is needed,25units of
regular insulin are added to 25mg of normal saline
The IV rate and supplimantal regular insuline based
on every 1to2 hr capillary boold glucose value
INTERMITENT SUBCUTINEOUS INSULIN